
Personalized CRISPR Remission™ for ME/CFS: State-Dependent Gene Editing in a Flare Responsive Neuroimmune Disease
- Apr 11
- 47 min read
Updated: May 7
This paper is part of the CYNAERA CRISPR Remission™ Library, a growing resource, impacting how gene editing is applied to neuro-immune and infection associated chronic conditions through personalized CRISPR gene editing pathways.
By Cynthia Adinig
Executive Summary
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a complex neuroimmune disease defined by profound physiologic instability rather than a fixed baseline. As Anthony Komaroff and W. Ian Lipkin have emphasized, the illness involves ongoing dysregulation across immune, metabolic, neurologic, and autonomic systems, producing a disease course shaped by fluctuation, relapse, and disproportionate response to stressors (Komaroff and Lipkin, 2021). Post-exertional malaise, described extensively by Leonard Chu, Leonard Jason, and Lucinda Bateman, illustrates this instability clearly: even minor exertion can trigger delayed and severe symptom worsening (Chu et al., 2019; Jason et al., 2011; Bateman et al., 2021).
Despite this, most intervention models still treat ME/CFS as though it were biologically stable. Patients are grouped into broad cohorts, therapies are applied without regard to timing or system readiness, and inconsistent outcomes are often interpreted as treatment failure rather than evidence of unmodeled variability. The problem is not simply a lack of biologic insight. Research led by Robert Naviaux, Maureen Hanson, Nancy Klimas, and others has already identified abnormalities across metabolism, immune signaling, and physiologic regulation (Naviaux et al., 2016; Hanson et al., 2016; Klimas et al., 2012). The missing piece is a framework capable of integrating those findings into intervention logic.
This paper introduces Personalized CRISPR Remission™ as a state-dependent gene-editing framework for ME/CFS. Rather than treating CRISPR as a one-time static correction, this model aligns target selection and intervention timing with phenotype, biologic context, and system readiness. It integrates phenotype-stratified cohort design, environmental and flare-state modeling through systems such as VitalGuard™, structured stabilization through the STAIR: Stable Method™, and patient-specific simulation through CYNAERA’s chronic condition digital twins. In this architecture, gene editing is first evaluated within a dynamic representation of the patient’s system rather than inferred from diagnosis alone.
Personalized CRISPR Remission™ therefore functions not only as a CRISPR framework, but as a broader platform for remission-oriented biologic intervention in complex disease, including other advanced strategies shaped by timing, immune environment, and terrain readiness. Together with CYNAERA’s phenotyping, environmental modeling, and stabilization frameworks, this approach outlines a full-stack architecture for state-dependent clinical trial design in ME/CFS. It provides a scalable and system-aligned pathway toward remission-oriented intervention, where variability becomes interpretable, therapeutic signal becomes detectable, and precision gene editing moves closer to enabling durable remission and, ultimately, cure.
This framework was introduced in abstract form at CRISPRMED26, reflecting growing recognition within the gene-editing field that intervention timing, system stability, and patient-specific variability are critical determinants of therapeutic success in complex disease.

1. ME/CFS as a State-Dependent System
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is best understood as a state-dependent, multi-system illness in which immune dysregulation, metabolic impairment, autonomic instability, and neurocognitive dysfunction interact dynamically over time. Rather than operating around a stable baseline, the disease shifts across periods of relative stability and destabilization in response to exertion, infection, environmental exposure, hormonal change, and other internal or external stressors (Institute of Medicine, 2015; Komaroff and Lipkin, 2021).
This complexity is paired with scale that remains widely underrecognized. While older prevalence estimates placed ME/CFS in the low millions in the United States, CYNAERA’s 2026 US-CCUC™ (U.S. Chronic Condition Undercount Correction) framework suggests a substantially larger burden, with approximately 27.5M–34.65M U.S. adults meeting ME/CFS classification criteria and a more conservative public-facing range of ~18M–26M adults. This reframes ME/CFS not as a rare or niche condition, but as a mass-scale chronic illness whose instability has been underestimated both biologically and epidemiologically.
Post-exertional malaise (PEM) represents the clearest clinical expression of this system behavior. Even minor physical or cognitive effort can trigger delayed and disproportionate worsening that persists for days or longer, indicating that system response depends not only on the trigger itself, but on the physiologic state in which that trigger occurs (Chu et al., 2019; Walitt et al., 2024). This pattern reflects nonlinear system dynamics, where identical inputs can produce markedly different outcomes depending on underlying system conditions.
This variability is not random. It reflects coordinated dysfunction across multiple systems, including immune signaling, metabolic regulation, autonomic control, and neurocognitive processing. Evidence from metabolomic, immunologic, and neuroimaging studies suggests that these systems do not operate independently, but interact dynamically, with disruptions in one domain propagating across others (Naviaux et al., 2016; Hanson et al., 2016; Lee et al., 2023). Within CYNAERA’s Unified Collapse Theory, this behavior is understood as a state-dependent system in which instability in one domain increases vulnerability across the entire network, amplifying the impact of subsequent stressors.
As a result, ME/CFS does not present as a uniform condition. Patients move between states of relative stability and acute deterioration, often without clear external markers. This has significant implications for both research and intervention. Approaches that assume a consistent baseline risk misinterpreting disease behavior, masking meaningful biologic signals, and obscuring treatment effects that are dependent on timing and system readiness. Patients have adapted to this reality in ways that reflect an implicit understanding of system dynamics. Pacing, buffering exertion, controlling environmental exposure, and adjusting activity based on early symptom signals are not incidental behaviors. They are strategies developed to manage variability within a highly sensitive system. However, these strategies have not been systematically incorporated into clinical trial design or therapeutic modeling.
Recognizing ME/CFS as a state-dependent system reframes the problem. It shifts the focus from identifying a single causal pathway to understanding how multiple interacting systems behave under varying conditions. Within this context, intervention outcomes are not determined solely by the nature of the treatment, but by when and how that treatment is introduced into the system. Timing, context, and physiologic readiness become central variables rather than secondary considerations. This shift establishes the foundation for a different approach to therapeutic design, one in which variability is not treated as noise, but as a defining feature of the disease that must be explicitly modeled.
2. Why Static Intervention Models Fail in ME/CFS
Traditional biomedical intervention models are built on an implicit assumption of physiologic stability. Patients are diagnosed, enrolled, and treated as if their underlying state is sufficiently consistent to allow for uniform intervention and evaluation. In ME/CFS, this assumption does not hold. As Anthony Komaroff and W. Ian Lipkin have emphasized, the illness reflects ongoing, multi-system dysregulation rather than a static disease state, with immune, neurologic, and metabolic abnormalities that fluctuate over time (Komaroff and Lipkin, 2021).
This instability is most clearly demonstrated through post-exertional malaise (PEM), which Leonard Jason and Lucinda Bateman, among others, have identified as the defining feature of ME/CFS. As Leonard Chu and colleagues showed in detailed patient cohorts, even minor exertion can trigger delayed and prolonged symptom exacerbation, reflecting a system in which response is dependent on prior state rather than proportional to input (Chu et al., 2019; Jason et al., 2011; Bateman et al., 2021). This nonlinear behavior challenges the core assumptions of traditional trial design, where interventions are expected to produce consistent effects across participants and timepoints.
The consequences of this mismatch are visible across decades of clinical trials. Øystein Fluge and Olav Mella’s work on rituximab, for example, demonstrated early promise in subset responses but ultimately failed to show consistent benefit in larger trials, highlighting the difficulty of detecting signal in heterogeneous populations (Fluge and Mella, 2019). Similarly, Suzanne Vernon and the Bateman Horne Center have emphasized that variability in patient presentation and timing contributes to inconsistent outcomes, even when biologic targets are plausible (Bateman et al., 2021). These failures are often interpreted as evidence against specific interventions, when in many cases they reflect misalignment between trial design and disease dynamics.
At the same time, the field has not lacked data. Research spanning metabolomics, immunology, and neurobiology has identified reproducible abnormalities across patient populations. Robert Naviaux’s metabolomic work has demonstrated a hypometabolic state consistent with a dauer-like response, while Maureen Hanson and colleagues have identified altered energy metabolism and immune signaling in ME/CFS cohorts (Naviaux et al., 2016; Hanson et al., 2016). Neuroimaging studies led by researchers such as Dikoma Shungu and more recently Avindra Nath and Michael VanElzakker have pointed to neuroinflammatory and central network dysfunction (Natelson et al., 2021; VanElzakker et al., 2019). Yet these findings have not translated cleanly into successful interventions, not because the biology is absent, but because it is not being applied within a model that accounts for temporal and state-dependent variability. As detailed in CRISPR Cas9 Immunity and Gene Editing Failure, immune response to Cas9 should be understood as dynamic and context-dependent rather than binary.
Patients, however, already behave as if these variables matter. Strategies such as pacing, buffering travel with rest days, scheduling IV hydration around high-demand events, adjusting medication dosing with clinician guidance, and avoiding new environmental or physiologic stressors prior to exertion are widely used to reduce symptom volatility. These patterns have been described qualitatively across patient-led and clinical communities, including work highlighted by Leonard Jason and others on illness management strategies (Jason et al., 2013). They represent a consistent, experience-driven system for managing timing, exposure, and physiologic load that has not yet been formally incorporated into clinical models.
The failure of static intervention models in ME/CFS is therefore not simply a failure of treatment. It is a failure to account for the dynamic conditions under which treatment is delivered. Without integrating state, timing, and environmental context, even well-targeted interventions risk producing variable and uninterpretable results.
3. Phenotype-Stratified Intervention Design in ME/CFS
Any intervention framework in ME/CFS must begin with heterogeneity as a defining characteristic of the disease. Patients differ across immune activation, metabolic capacity, autonomic regulation, neurocognitive function, hormonal signaling, and environmental sensitivity, resulting in multiple overlapping but distinct phenotypic states. Anthony Komaroff has long emphasized the multi-system nature of ME/CFS, while more recent work from Brian Walitt and colleagues highlights the variability in symptom expression and trajectory across patient populations (Komaroff and Lipkin, 2021; Walitt et al., 2024).
Despite this, research has historically treated ME/CFS as a single entity, collapsing biologically distinct patients into unified cohorts. The Institute of Medicine’s 2015 report acknowledged this heterogeneity while also noting the lack of structured stratification in both research and clinical care (Institute of Medicine, 2015). This limitation has been repeatedly identified as a barrier to progress, as meaningful differences in biology and response are obscured when patients are grouped without regard to underlying system involvement.
Within the Personalized CRISPR Remission™ framework, phenotyping functions as the critical bridge between target selection and intervention timing. Rather than assigning interventions based solely on diagnosis, patients are stratified according to dominant system involvement and current physiologic state. This aligns with broader precision medicine approaches, but extends them by incorporating temporal dynamics and environmental interaction, elements that are particularly relevant in ME/CFS.
Within this model, phenotype is not a fixed label, but a dynamic state defined by core system involvement and trigger interaction. This approach is formalized in the CYNAERA 25 Core ME/CFS Phenotyping Framework, where phenotype is defined as:
Phenotype = Core Axis × Trigger/Modulator + Functional Signature
This formulation reflects the reality that ME/CFS is shaped not only by baseline biology, but by how that biology responds to exertion, infection, hormonal shifts, and environmental exposure. Work from researchers such as Maureen Hanson and Nancy Klimas has demonstrated that immune and metabolic responses in ME/CFS are highly context-dependent, shifting in response to stressors and time (Hanson et al., 2016; Klimas et al., 2012). Similarly, autonomic research led by Satish Raj and Julian Stewart has shown that circulatory and cardiovascular responses vary significantly across patients, contributing to distinct clinical presentations (Raj et al., 2021).
Core phenotypic domains include energy dysregulation, autonomic and circulatory function, neuroimmune and sensory processing, hormonal and endocrine regulation, immune and reactivation patterns, and sleep and pain architecture. In addition, social and structural modifiers play a significant role in shaping disease trajectory. Research on health disparities, including work by Monica Webb Hooper and others, has demonstrated that access to care, misdiagnosis, and socioeconomic factors influence both diagnosis and outcomes in chronic illness populations (Wong et al., 2023). These factors are not external to the disease. They interact with biologic systems to influence severity, progression, and response to intervention.
These domains are not mutually exclusive. Patients frequently exhibit multi-axis involvement and may shift between phenotypic states over time, reinforcing the need for dynamic classification rather than static subgrouping. This variability has direct implications for intervention design. An immune-dominant phenotype may require stabilization prior to immune-targeted editing, while a metabolic-dominant phenotype may have limited tolerance for interventions that depend on energy-intensive repair processes. Autonomic-dominant phenotypes require alignment with cardiovascular stability, and neuroimmune phenotypes require consideration of sensory and cognitive load.
This approach aligns with CYNAERA’s broader modeling systems, including SymCas™ for flare prediction and the Pathos framework for severity classification, which integrate symptom patterns, physiologic signals, and temporal dynamics to characterize system state. By combining phenotypic stratification with state-dependent modeling, intervention strategies can be matched to both the underlying biology and the current condition of the system.
The implications for clinical trial design are substantial. Trials that do not incorporate phenotypic stratification risk grouping biologically distinct patients into the same cohort, diluting signal and contributing to repeated failure. By contrast, phenotype-stratified design enables more precise cohort selection, improved alignment between intervention and biology, and a higher likelihood of detecting meaningful therapeutic effects, a point emphasized across trial and cohort design literature (Fluge and Mella, 2019; Bateman et al., 2021).
A full phenotypic classification system, including domain-level scoring, subtype differentiation, and dynamic state tracking, is detailed in the CYNAERA phenotyping framework. That system provides the structural basis for cohort design, intervention matching, and adaptive clinical trial structure referenced throughout this paper.
Phenotype-Stratified Trial Design Implications
The integration of phenotyping, state-dependent modeling, and environmental alignment has direct implications for clinical trial design in ME/CFS. Rather than enrolling patients based solely on diagnosis, participants can be stratified into phenotype-aligned cohorts reflecting dominant system involvement, including immune, metabolic, autonomic, neuroimmune, and multi-system presentations.
Within this structure, intervention design is adapted across cohorts:
immune-dominant phenotypes are aligned with immune-modulating targets and low-inflammatory timing windows
metabolic-dominant phenotypes require energy-stable conditions and avoidance of post-exertional states
autonomic-dominant phenotypes require cardiovascular stabilization and timing aligned with physiologic stability
neuroimmune phenotypes require low sensory and neuroinflammatory load states
multi-system phenotypes require extended stabilization prior to intervention
Across all cohorts, intervention timing is guided by state-dependent modeling and environmental conditions, incorporating frameworks such as VitalGuard™ and the STAIR: Stable Method™ to align treatment with periods of maximal system readiness. A detailed phenotype-stratified trial architecture, including cohort definitions, target alignment, and timing protocols, is provided in the Appendix.

4. Real-World State Contrast in ME/CFS
To demonstrate how terrain alters intervention outcomes, consider a single patient with an autonomic-metabolic phenotype characterized by post-exertional malaise, orthostatic intolerance, cognitive dysfunction, and intermittent inflammatory activation. Genetic and multi-omic review suggests relevance of targets such as NAMPT, ACE, and IL12A across metabolic, vascular-autonomic, and immune domains (Walitt et al., 2024; Zhang et al., 2025).
These terrain shifts are consistent with the Unified Collapse Theory, in which dysfunction across metabolic, autonomic, immune, and neurocognitive domains does not occur in isolation but propagates across systems. In this model, a perturbation in one domain, such as exertion or environmental stress, can amplify instability in others, producing the nonlinear and state-dependent symptom patterns observed in ME/CFS.
Table 1. Same Patient, Different Terrain: State-Dependent Editing Outcomes in ME/CFS
Dimension | Scenario A: Post-Flight PEM | Scenario B: Post–Category 3 Hurricane Flare | Scenario C: Pre-Stabilized Window Using Patient-Led Terrain Optimization |
Primary context | Long flight → PEM and autonomic strain | Barometric shift + environmental instability and exposure burden | Buffered travel + IV hydration + medication adjustment + exposure control + baseline stabilization |
Dominant terrain | Metabolic depletion + autonomic instability | Environmental burden + inflammatory amplification | Controlled exertion + preserved baseline + minimized variability |
Immune state | Acute, exertion-driven fluctuation | Sustained, exposure-linked activation | Reduced volatility through trigger avoidance |
Metabolic capacity | Low reserve, impaired recovery | Suppressed by stress, sleep disruption | Preserved through pacing and hydration |
Autonomic stability | Highly unstable | Persistently dysregulated | Supported via hydration and beta-blocker adjustment |
Environmental load | Moderate, unmanaged | High, multi-factor exposure | Actively mitigated via HEPA filtration and masking |
Baseline variability | High | High | Minimized through avoidance of new inputs |
Editing readiness | Low | Low–moderate | Moderate–high if stability maintained |
Outcome (static model) | Inconclusive | Noisy | Missed advantage |
Outcome (state-dependent model) | Deferred | Delayed | Timed for signal detection |
Interpretation
Across these scenarios, the patient and targets remain constant, yet the intervention conditions differ substantially. In the post-flight state, metabolic depletion and autonomic instability dominate, limiting the system’s ability to tolerate additional perturbation. In the post-hurricane state, environmental burden, disrupted recovery, and exposure-sensitive inflammatory amplification reshape the terrain, altering target relevance and increasing response variability. In the pre-stabilized scenario, patient-led strategies such as paced travel, hydration support, medication adjustment, exposure control, and baseline stabilization reduce volatility and preserve physiologic reserve, creating a more interpretable window for intervention (Chu et al., 2019; Walitt et al., 2024).
What appears as inconsistent response in these settings is not random variation, but the consequence of unmodeled terrain differences across immune, metabolic, autonomic, and environmental domains. In this sense, observed variability can be understood as the expression of a system operating near instability thresholds, where relatively small changes in input, such as exertion, travel stress, barometric shifts, or exposure burden, produce disproportionately large changes in output. When these differences are ignored, therapeutic signal is lost. When they are incorporated into intervention logic, outcome patterns become more interpretable and biologically coherent (Chu et al., 2019; Lee et al., 2023; Walitt et al., 2024).
Illustrative Patient Scenario: From Instability to Intervention Readiness
A single patient with ME/CFS presents with a predominantly autonomic-metabolic phenotype, characterized by post-exertional malaise, orthostatic intolerance, cognitive dysfunction, and episodic inflammatory flares. Under standard care conditions, the patient’s baseline state is highly variable. Daily function fluctuates, exertion leads to delayed crashes, and environmental triggers such as travel, poor air quality, or barometric shifts produce disproportionate worsening. Despite appropriate target identification, including pathways related to metabolic regulation, immune signaling, and vascular stability, intervention outcomes remain inconsistent.
In this baseline state, intervention is applied without alignment to system conditions. Following a long flight, the patient enters a post-exertional malaise phase marked by metabolic depletion, autonomic instability, and impaired recovery capacity. In this context, even well-targeted intervention is introduced into a system operating near its tolerance threshold. The result is not necessarily adverse, but it is difficult to interpret. Response is variable, symptom burden increases, and signal is obscured by underlying instability.
A similar pattern emerges following environmental stress. After a major storm event with significant barometric fluctuation and indoor exposure burden, the patient experiences sustained inflammatory activation and worsened autonomic dysfunction. The same intervention applied in this context produces a different pattern of response, not because the target has changed, but because the terrain has shifted. What appears as inconsistency is, in reality, the predictable outcome of unaligned intervention within a multi-system, state-dependent condition.
By contrast, when the same patient undergoes structured pre-intervention stabilization, the system behaves differently. Travel is buffered with rest days before and after, IV hydration is used to support circulatory stability, medication dosing is adjusted in coordination with clinicians, environmental exposure is actively managed, and new variables are minimized in the days leading up to intervention. These measures reduce system load and preserve baseline function. In this stabilized state, intervention is introduced within a narrower and more controlled physiologic range. Autonomic variability is reduced, metabolic reserve is improved, and inflammatory fluctuation is minimized. The system remains responsive, but no longer operates at the edge of tolerance. Under these conditions, the same therapeutic input produces a more consistent and interpretable response.
The difference between these scenarios is not the patient and not the intervention. It is the condition of the system at the time of application. This contrast illustrates a central principle of the Personalized CRISPR Remission™ framework: intervention success in ME/CFS is determined not only by what is targeted, but by when and under what conditions the intervention is applied.

5. Safety, Timing, and Delivery in Gene-Based Intervention
The translation of CRISPR-based therapies into ME/CFS requires careful consideration of safety, delivery, and biological timing. While advances in gene editing have improved precision, risks remain, particularly in conditions defined by immune variability, autonomic instability, and multi-system interaction. In this context, safety cannot be understood as a fixed property of the therapeutic alone, but as a function of the interaction between the intervention and the system state at the time it is applied.
One of the primary concerns in CRISPR-based intervention is off-target modification, where unintended genomic edits may occur. Advances in guide RNA design, base editing, and prime editing have significantly reduced this risk, but it remains a central consideration, particularly in complex conditions where small perturbations can have amplified downstream effects (Doudna, 2020; Chen et al., 2024). In ME/CFS, where immune, neurologic, and metabolic pathways are tightly coupled, unintended modulation may have system-wide consequences rather than isolated effects.
Immunogenicity represents an additional constraint. Delivery vectors and CRISPR-associated proteins can trigger immune responses, potentially reducing therapeutic effectiveness or introducing adverse effects (Naldini, 2015). In a condition already characterized by immune dysregulation and fluctuating inflammatory activity, this risk is amplified when intervention is applied during periods of elevated system load.
Delivery remains a major technical barrier. Targeting relevant tissues, including central nervous system structures, autonomic pathways, and peripheral immune compartments, requires precise and controlled delivery systems. Viral vectors such as adeno-associated viruses have demonstrated promise, but limitations in tissue specificity and immune activation persist. Emerging non-viral delivery systems, including lipid nanoparticles, offer potential advantages but require further refinement for multi-system targeting (Pardi et al., 2018; Habib et al., 2023).
A critical distinction in ME/CFS is the importance of regulation rather than permanent disruption. Unlike monogenic diseases where permanent correction is desirable, ME/CFS involves fluctuating and interdependent system behavior. As a result, the Personalized CRISPR Remission™ framework prioritizes regulatory approaches, including CRISPR interference (CRISPRi) and CRISPR activation (CRISPRa), which allow for controlled modulation of pathways rather than irreversible elimination.
Table 2. State-Dependent Safety Mapping Framework
To clarify how system state influences safety and response, the relationship between system load, regulatory capacity, and intervention behavior can be represented as a structured mapping:
Phenotype | Baseline System Load L(t) | Regulatory Capacity T | Threshold Margin (T − L) | Intervention Behavior | Safety Risk Profile |
Immune-dominant | Elevated inflammatory signaling | Constrained | Narrow or negative | Amplifies immune response | High risk of inflammatory events |
Neuroimmune-dominant | Moderate load, high neural sensitivity | Variable | Narrow, unstable | Triggers central sensitization | Cognitive and neurologic symptoms |
Autonomic-dominant | Fluctuating load, vascular instability | Labile | Rapidly shifting | Destabilizes autonomic balance | Tachycardia, hypotension, syncope |
Mixed / IACC | Multi-domain elevated load | Globally reduced | Minimal or negative | Cross-system competition | Unpredictable multi-system response |
Stabilized State (Post-STAIR) | Reduced, controlled load | Improved | Positive and sustained | Processed within tolerance | Lower risk, consistent response |
Interpretation
This framework demonstrates that safety in ME/CFS is not determined solely by the intervention itself, but by the relationship between system load and regulatory capacity at the time of intervention. When baseline load is elevated and threshold margin is compressed, even low-dose or precisely targeted interventions may function as destabilizing inputs. This aligns with allostatic load theory, in which cumulative system burden reduces adaptive capacity and increases sensitivity to additional stressors (McEwen, 2007; Sterling, 2012).
In immune-dominant states, elevated cytokine signaling amplifies response to intervention, increasing the risk of inflammatory adverse events. In neuroimmune-dominant states, altered central processing increases susceptibility to neurologic and cognitive effects, even when peripheral markers are stable (Ji et al., 2018). Autonomic-dominant states introduce additional instability through vascular and regulatory fluctuation, increasing risk of tachycardia, hypotension, and syncope (Goldstein, 2020).
By contrast, in stabilized states where system load is reduced and regulatory capacity is improved, the threshold margin widens. This allows therapeutic input to remain within system tolerance, resulting in more predictable engagement and reduced adverse response. This pattern is consistent with desensitization and graded exposure models observed in mast cell and hypersensitivity disorders (Castells, 2017; Weinstock et al., 2021).
Key Insight
The transition from unsafe to safe intervention does not require a change in the therapeutic itself. It requires a shift in system conditions such that:
U(t) + L(t) < T
Where:
U(t) = intervention input
L(t) = baseline system load
T = regulatory capacity
This reframes safety as a dynamic system property, not a static attribute of the intervention. Timing integrates all of these variables. Intervention applied during instability increases risk and reduces interpretability. Intervention aligned with stabilization windows improves both safety and durability. Safety, therefore, emerges from alignment between intervention, system state, and delivery context.
6. CRISPR Remission™ as a State-Dependent Intervention Framework
The Personalized CRISPR Remission™ framework addresses these limitations by reframing gene editing as a process that must be aligned with biological state rather than applied as a uniform correction. In this model, CRISPR is not treated as a one-time intervention but as part of a broader system in which the timing, context, and conditions of delivery determine whether an intervention contributes to stabilization or further destabilization of the system. This perspective reflects a growing recognition that gene-editing outcomes are influenced not only by target selection, but by delivery context, immune environment, and system-level conditions at the time of intervention (Doudna and Charpentier, 2014; Naldini, 2015).
In ME/CFS, this requires a shift from target-centric thinking to terrain-aware modeling, where molecular targets are evaluated within the context of the patient’s current physiological state. This includes consideration of immune activation levels, metabolic capacity, autonomic regulation, neurocognitive function, and environmental exposures, all of which influence how the system responds to intervention. Rather than assuming that modifying a given gene will produce a consistent outcome, this framework recognizes that the same intervention may have different effects depending on whether the system is in a stable phase, a post-exertional crash, or a period of ongoing immune activation (Chu et al., 2019; Komaroff and Lipkin, 2021; Walitt et al., 2024).
This state-dependent variability is supported by a growing body of ME/CFS research. Studies have demonstrated that exertional stress can trigger widespread metabolic and immunologic shifts, including altered energy metabolism, oxidative stress, and inflammatory signaling, all of which can influence system responsiveness to additional perturbation (Naviaux et al., 2016; Hanson et al., 2016). Neuroimaging and systems-level analyses further suggest that central nervous system involvement and network-level dysfunction contribute to disease expression and variability, reinforcing the need to consider intervention timing in relation to system-wide coordination rather than isolated pathways (Lee et al., 2023; Shan et al., 2020). Autonomic dysfunction, including impaired cardiovascular regulation and orthostatic intolerance, introduces an additional layer of instability that can influence both safety and interpretability of intervention outcomes (Natelson et al., 2021).
Within this structure, intervention design becomes inherently customized and individualized, as targets are selected and applied based on phenotype, system stability, and readiness for intervention. Consistent with CYNAERA’s SymCas™ flare prediction model and the CYNAERA Science to Remission white paper, the concept of terrain readiness is central, meaning that interventions are prioritized not only by biological relevance but by whether the system is capable of tolerating and responding to modification at a given point in time. This aligns with broader precision medicine approaches while extending them into a dynamic, state-aware framework that accounts for temporal variability rather than static patient characteristics.
To operationalize this approach, the framework integrates multiple domains of biological and environmental information:
immune signaling patterns and inflammatory burden as indicators of system activation and risk of adverse response (Hanson et al., 2016)
metabolic capacity and mitochondrial function as constraints on energy-dependent repair and recovery processes (Naviaux et al., 2016)
autonomic stability as a measure of regulatory balance and physiological resilience (Natelson et al., 2021)
neurocognitive and central network function as contributors to both symptom expression and systemic coordination (Lee et al., 2023)
environmental exposure as a modulator of symptom volatility and flare risk (Chu et al., 2019)
CRISPR success in ME/CFS is state-dependent, not diagnosis-dependent. By aligning gene-editing strategies with these variables, the CRISPR Remission™ framework provides a pathway for translating complex, heterogeneous data into actionable intervention strategies that are responsive to the dynamic nature of the disease. This approach does not eliminate uncertainty, but it reduces misalignment between intervention and system state, increasing the likelihood that gene editing can contribute to meaningful and durable remission in ME/CFS.
Digital twin modeling provides the operational layer for this framework. Within CYNAERA’s architecture, chronic condition digital twins simulate individual patient states across immune, metabolic, autonomic, and environmental domains, allowing prospective evaluation of how specific gene-target interventions may interact with a given system. Rather than selecting targets based on diagnosis alone, this approach enables state-aware testing of intervention timing, pathway modulation, and flare risk prior to real-world application. In this model, CRISPR is not applied to a patient. It is first evaluated within a dynamic representation of that patient’s system.
7. Candidate Gene Classes and Editing Strategy for ME/CFS
Within a state-dependent framework, candidate genes are not only defined by their association with disease, but by how they can be modulated, stabilized, or rebalanced under specific biological conditions. In ME/CFS, this requires moving beyond identification toward intervention logic, where each target is evaluated in terms of its role in system instability, its responsiveness to modulation, and the conditions under which editing is most likely to support recovery rather than exacerbate dysfunction.
Emerging genetic and multi-omic work suggests that ME/CFS is shaped by polygenic disruption across immune, metabolic, autonomic, and neurocognitive systems, rather than a single causal mutation (Klaassen et al., 2025; Wiborg et al., 2023). This supports a model in which gene editing is not deployed as a one-time correction, but as a targeted modulation strategy across multiple domains, each requiring different approaches depending on phenotype and state. To make this concrete, the following table outlines both representative targets and proposed editing logic, aligning each gene with a functional intervention strategy rather than a static label.
Table 3. State-dependent gene-editing strategies in ME/CFS
Terrain domain | Gene | Dysfunction pattern | Proposed editing approach | State-dependent consideration |
Metabolic / mitochondrial | NAMPT | Reduced NAD availability, impaired energy metabolism, low recovery capacity | Upregulation via CRISPRa or pathway activation to restore NAD biosynthesis and improve metabolic resilience | Best applied during relative metabolic stability, not during acute PEM or energy collapse |
Immune-inflammatory | IL12A | Dysregulated cytokine signaling, excessive or unstable inflammatory activation | Downregulation or modulation via CRISPRi to reduce inflammatory burden without suppressing immune defense | Requires distinction between inflammatory vs immunosuppressed phenotypes |
Autonomic / vascular | ACE | Impaired vascular tone, autonomic imbalance, circulatory instability | Modulation rather than full suppression, adjusting signaling balance to stabilize autonomic response | Timing sensitive to orthostatic instability and cardiovascular stress states |
Proteostasis / immune processing | PSMB4, PSMB5, PSMD7 | Impaired protein degradation, chronic immune activation, cellular stress accumulation | Functional stabilization or partial modulation to improve protein turnover and immune recalibration | Likely most relevant in chronic inflammatory or post-trigger persistence phases |
Neurocognitive / synaptic | SYNGAP1 | Disrupted synaptic signaling, cognitive dysfunction, impaired network regulation | Targeted modulation rather than direct editing, potentially through upstream regulatory pathways | High sensitivity to system instability, requires strong baseline stabilization before intervention |
What unites these target classes is not that they sit in the same pathway, but that they each map onto a domain of instability already visible in ME/CFS literature. In that sense, the paper is not proposing that ME/CFS should be edited gene by gene in a flat or universal way. It is proposing that state-dependent intervention requires molecular nodes that can be interpreted within terrain, meaning their relevance depends on phenotype, biologic readiness, and the wider system in which they are being modified. This is also why the broader modeling appendix matters. The purpose of the smaller set in the main paper is to establish logic, while the larger modeled set demonstrates that this is not a thought experiment but a scalable prioritization structure.

8. Environmental Modeling and Flare-State Constraints on Gene Editing
In ME/CFS, environmental exposure and flare-state dynamics function as active constraints on intervention, not passive background variables. This includes not only air pollutants such as particulate matter, ozone, and wildfire smoke, but also atmospheric instability itself, including barometric pressure shifts, humidity load, dew point elevation, temperature variability, and post-storm indoor air degradation. In a condition marked by immune activation, metabolic constraint, and autonomic instability, these variables can alter the biologic terrain before any therapeutic input is introduced, directly affecting whether a gene-editing intervention is feasible, interpretable, or destabilizing (Chu et al., 2019; Komaroff and Lipkin, 2021; Mukamal et al., 2009; Vertigan et al., 2016).
This aligns with a broader body of environmental health research demonstrating that pollutant exposure activates inflammatory pathways, increases oxidative stress, and disrupts autonomic and cardiovascular regulation. Fine particulate matter and ozone are associated with increased respiratory and cardiovascular events, while humidity and pressure shifts are linked to neurologic and autonomic instability (Dominici et al., 2006; Pope et al., 2019). Post-storm dampness, mold proliferation, and degraded indoor air quality are further associated with sustained inflammatory burden and worsening fatigue trajectories (Fisk et al., 2010; Park et al., 2006). These biological effects converge on mechanisms that overlap with core features of ME/CFS, including mitochondrial dysfunction, neuroinflammation, immune dysregulation, and autonomic instability (National Academies of Sciences, 2015; Komaroff and Lipkin, 2021).
Atmospheric and Weather-Linked Drivers of Instability
Not all environmental triggers in ME/CFS are pollutant-based. Atmospheric variables such as barometric pressure change, humidity burden, dew point elevation, rapid temperature shifts, and storm-linked indoor dampness can independently alter system stability. These conditions influence autonomic regulation, vascular tone, respiratory function, and neurologic sensitivity, and are associated with increased migraine activity, cardiovascular strain, and dysautonomic symptoms in vulnerable populations (Mukamal et al., 2009; Vertigan et al., 2016).
For patients with ME/CFS and overlapping conditions such as POTS, Lyme, mast cell activation syndrome, or chemical sensitivity, these atmospheric shifts can amplify baseline instability. A rapid pressure drop preceding a storm, a sustained high-dew-point heat event, or post-flood indoor air degradation can each move the system into a higher-load state before additional exposures or exertion are introduced. In this context, atmospheric conditions function as pre-loading factors, shaping intervention readiness prior to any direct therapeutic input.
Mechanistic Environmental Drivers of Flare-State Instability
Environmental exposures relevant to ME/CFS are not uniform. Distinct pollutant classes activate different biological pathways, many of which intersect directly with the pathophysiology of infection-associated chronic conditions.
Polycyclic aromatic hydrocarbons (PAHs), present in diesel exhaust, wildfire smoke, and urban pollution, activate the aryl hydrocarbon receptor (AhR), contributing to cytokine imbalance, mitochondrial stress, and endocrine disruption (Boström et al., 2002; Kim et al., 2013). Particulate matter (PM₂.₅ and PM₁₀) penetrates pulmonary and vascular systems, triggering systemic inflammation, oxidative stress, and endothelial dysfunction through pathways such as NF-κB activation and cytokine release (Pope et al., 2016; Gawda et al., 2018).
Traffic-related pollutants such as nitrogen dioxide (NO₂) impair immune function and increase airway inflammation, while ozone (O₃) acts as a potent oxidant, inducing epithelial injury and systemic stress responses (Ciencewicki and Jaspers, 2007; Hollingsworth et al., 2007; World Health Organization, 2022). Volatile organic compounds (VOCs), including benzene, formaldehyde, and toluene, introduce neurotoxic and inflammatory stress and are associated with mast cell activation and autonomic instability (ATSDR, 2020; Drzazga et al., 2021; Hanna et al., 2021). These exposures do not act independently. They contribute to a cumulative environmental burden that can shift the system toward instability, increasing flare probability and reducing tolerance for additional perturbation.
Table 4: Environmental and Atmospheric Drivers of ME/CFS Flare Instability and Intervention Constraints
Environmental Trigger | Common Sources or Conditions | Biological Mechanisms | Implication for Gene Editing |
Barometric pressure shifts | Storm fronts, hurricanes, rapid weather changes | Autonomic instability, vascular stress, neurologic sensitivity | Reduced physiologic stability, increased variability in intervention response |
Humidity / high dew point | Heat waves, coastal weather, post-storm conditions | Thermal stress, autonomic burden, respiratory strain | Lower tolerance for intervention, increased system load |
Temperature variability | Heat spikes, cold fronts, seasonal instability | Cardiovascular strain, metabolic stress | Increased baseline instability, reduced interpretability of response |
Mold / dampness | Water damage, flooding, poor ventilation | Immune activation, mast cell signaling, cytokine production | Sustained inflammatory burden, interference with immune targeting |
PAHs | Diesel exhaust, wildfire smoke | AhR activation, cytokine imbalance, mitochondrial stress | Increased inflammatory volatility, reduced predictability |
PM₂.₅ / PM₁₀ | Traffic, industry, wildfire smoke | NF-κB activation, IL-6/TNF-α signaling, oxidative stress | Elevated system load, reduced tolerance for modulation |
NO₂ | Vehicle emissions | Airway inflammation, immune impairment | Increased inflammatory reactivity during intervention |
O₃ | Photochemical smog | Oxidative stress, epithelial injury | Amplified systemic stress, reduced intervention stability |
VOCs | Indoor air, off-gassing | Neurotoxicity, mast cell activation, autonomic disruption | Increased neurologic sensitivity and variability |
From Environmental Exposure to System Load
Within this framework, environmental input is not treated as isolated triggers but as a layered system of cumulative load. Atmospheric instability, pollutant exposure, indoor air quality, seasonal cycles, and regional vulnerability interact to produce a dynamic system burden that directly influences immune activation, metabolic capacity, and autonomic regulation. This aligns with models of cumulative stress and allostatic load, in which multiple inputs reduce regulatory capacity and increase sensitivity to additional perturbation (McEwen, 2007; Sterling, 2012). In ME/CFS, where baseline regulatory capacity is already constrained, this cumulative load can rapidly shift the system into instability.
Flare-State Dynamics as an Intervention Constraint
Flare-state dynamics further complicate this landscape. Post-exertional malaise represents a condition in which immune signaling, metabolic function, and autonomic regulation are simultaneously destabilized, creating conditions under which intervention response becomes highly variable (Chu et al., 2019). Delivering a gene-editing intervention during or immediately following a flare may obscure therapeutic signal, increase the risk of adverse response, or produce effects that do not generalize beyond that specific state. This introduces a practical requirement that intervention timing must be aligned with periods of relative biological stability, rather than convenience or static scheduling.
VitalGuard™ and Predictive Terrain Modeling
To operationalize this, environmental and flare-state modeling must be integrated into intervention planning as a gating mechanism. Within the Personalized CRISPR Remission™ framework, this is approached through terrain-based assessment, in which editing readiness is evaluated according to exposure burden, symptom trajectory, and physiologic stability. Consistent with CYNAERA’s VitalGuard™ framework, these variables can be modeled in real time to generate predictive assessments of intervention readiness. This includes barometric pressure change, humidity load, dew point, mold risk, particulate burden, ozone levels, wildfire smoke density, and localized housing degradation, all integrated with condition-specific sensitivity profiles.
The resulting model produces dynamic estimates of system instability:
Flare Score (t) = Σ [Eᵒ(t) × Wᵒ(c) × Rᵒ(g) × Sᵒ(s) × EQ] + M(t) + C(t) + L(t)
This enables identification of 48–72 hour windows of relative stability or elevated risk, allowing intervention timing to be aligned with biologic readiness rather than assumed baseline conditions.
Note on Terrain Response and Environmental Conditioning
The environmental modeling described here focuses on intervention timing and flare-state alignment in ME/CFS. Within CYNAERA’s broader architecture, this logic extends further into dynamic environmental conditioning through the Terrain Response Score (TRS), developed within the Microdosing Air™ framework.
Rather than relying on fixed exposure schedules, TRS evaluates whether a patient’s biologic terrain is sufficiently stable to tolerate environmental input by integrating terrain stability, autonomic resilience, barrier integrity, and trigger potency into a composite readiness score. In that system, low scores indicate that exposure should be deferred, moderate scores allow controlled microexposure, and higher scores support gradual expansion of tolerated environmental input. This distinction matters because environmental variables in CYNAERA are not only modeled as flare amplifiers, but also as conditioning inputs whose effects depend on the state of the underlying terrain. The gene-editing framework described in this paper draws on the same principle: system readiness must be established before additional biologic input can be expected to produce stable and interpretable outcomes.
Key Implication for Gene Editing
Environmental modeling is not an accessory to intervention design in ME/CFS. It is a primary determinant of system state. Barometric pressure, humidity, mold burden, particulate exposure, and cumulative environmental load function as biologically active intervention constraints, shaping whether the system can tolerate and respond to gene editing. Frameworks that do not incorporate these variables are likely to encounter avoidable variability, reduced interpretability, and diminished efficacy. By contrast, terrain-aware models such as VitalGuard™ enable a shift from reactive intervention to predictive, state-aligned deployment, where timing becomes as critical as target selection.
The strategies described above represent observable behaviors, but they do not constitute the full model. Within CYNAERA’s architecture, stabilization is formalized as a multi-phase system designed to reduce biologic volatility and align intervention with system readiness. Within CYNAERA’s Science of Remission framework, durable improvement is not achieved by forcing change within an unstable system, but by first establishing sufficient stability to support recovery processes. This reframes intervention from a direct corrective act to a coordinated, state-dependent process in which timing, terrain, and system readiness determine whether therapeutic inputs can be integrated and sustained.
This logic is consistent with the broader ME/CFS literature. Anthony Komaroff and W. Ian Lipkin have emphasized that ME/CFS reflects persistent multi-system dysfunction rather than a single stable lesion, while Leonard Chu and Brian Walitt have shown that disease expression is shaped by fluctuating autonomic function, post-exertional worsening, symptom variability, and subgroup-level biologic differences that complicate intervention timing and interpretation when left unmodeled (Komaroff and Lipkin, 2021; Chu et al., 2019; Walitt et al., 2024). Similarly, work from Lucinda Bateman and the Bateman Horne Center has reinforced the importance of stratification and symptom-linked disease management in a condition where patients do not behave as a uniform population (Bateman et al., 2021).
Neurobiologic and systems-level findings further support the need for a stabilization framework. Jason-Soo Lee, Woo Suck Sato, and Chang-Gue Son have shown through neuroimaging review and meta-analysis that ME/CFS involves networked dysfunction and neuroinflammatory change rather than isolated impairment, while Dikoma Shungu, Benjamin Natelson, and colleagues have described altered brain energetics, neuroinflammatory features, and physiologic dysregulation that reinforce the absence of a truly stable baseline (Lee et al., 2023; Natelson et al., 2021; VanElzakker et al., 2019). Robert Naviaux’s metabolomic work and Maureen Hanson’s immunologic findings similarly suggest that metabolic and immune systems in ME/CFS remain vulnerable to perturbation, supporting the idea that system readiness must be established before additional biologic input can be meaningfully evaluated (Naviaux et al., 2016; Hanson et al., 2016).
The STAIR: Stable Method™ defines stabilization as progressive alignment across immune signaling, metabolic capacity, autonomic regulation, and environmental exposure. In this model, readiness is not defined by symptom absence, but by the system’s ability to tolerate perturbation without cascading dysfunction. This distinction parallels broader theories of physiologic adaptation and cumulative stress. Bruce McEwen’s work on allostatic load and Peter Sterling’s model of predictive regulation both support the idea that repeated stress exposure narrows adaptive capacity, increasing the likelihood that additional inputs will produce disproportionate responses rather than controlled adaptation (McEwen, 2007; Sterling, 2012). In ME/CFS, where autonomic, immune, and metabolic reserve may already be constrained, stabilization becomes a prerequisite for interpretable intervention rather than an optional prelude.
Environmental tolerance operates in parallel. As demonstrated in the Microdosing Air™ framework, exposure does not function as a simple binary, but along a gradient in which system response depends on timing, intensity, and underlying stability. This has parallels in immunology and desensitization science. Cezmi Akdis and Mübeccel Akdis, along with Stephen Durham and Mohamed Shamji, have shown that graded exposure and tolerance induction depend on biologic context, dose, and immune readiness rather than exposure alone (Akdis and Akdis, 2011; Durham and Shamji, 2019). In mast cell and hypersensitivity-related conditions, Lawrence Afrin, Mariana Castells, and Peter Valent have likewise described threshold-dependent reactivity in which apparently minor exposures can trigger major responses when baseline system load is already elevated (Afrin et al., 2020; Castells, 2017; Valent et al., 2019). These principles reinforce the need for state-dependent environmental modeling in ME/CFS, where factors such as air quality, humidity, barometric pressure, mold burden, and cumulative exposure load can alter whether an intervention window is biologically tolerable.
These frameworks extend beyond visible tactics such as hydration, pacing, and avoidance. They integrate predictive modeling, flare-risk assessment, and environmental tracking to identify intervention windows aligned with system readiness, enabling more precise, personalized, and remission-oriented strategies. Without this structure, state-dependent intervention risks being reduced to isolated behaviors rather than understood as a coordinated and scalable system. The practical significance is clear: in ME/CFS, pre-intervention preparation is not ancillary to treatment. It is part of the mechanism by which treatment becomes interpretable, tolerable, and capable of producing durable remission.
10. Economic Impact and System-Level Value in ME/CFS
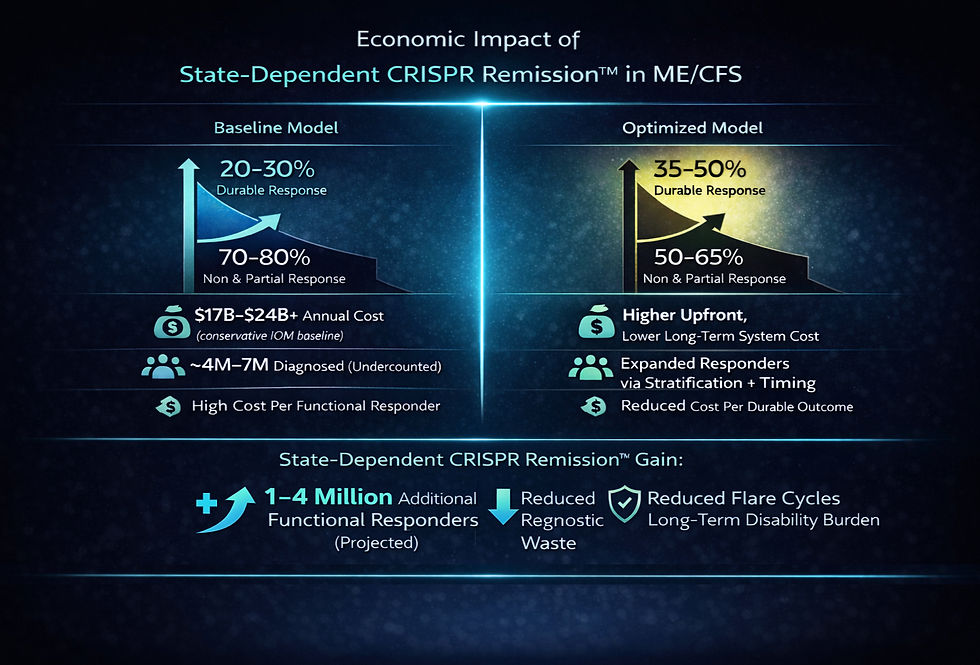
The economic burden of ME/CFS reflects not only the cost of illness, but the cost of repeated failure in diagnosis, treatment, and research translation. In a disease defined by biological instability and heterogeneity, interventions that are not aligned with system state are more likely to produce variable or inconclusive outcomes, contributing to wasted clinical trials, delayed therapeutic progress, and sustained underinvestment. As a result, a significant portion of the economic burden in ME/CFS is not intrinsic to the disease itself, but arises from misalignment between intervention design and the dynamic conditions of the system.
Published estimates provide a baseline for understanding this burden. The Institute of Medicine estimated that ME/CFS costs the U.S. economy approximately $17 billion to $24 billion annually through medical expenses and lost productivity, even under older prevalence assumptions that almost certainly undercounted the true affected population (Institute of Medicine, 2015). CYNAERA’s US-CCUC™ framework suggests that this undercount is substantial, with updated modeling placing ME/CFS classification burden at approximately 27.5M–34.65M U.S. adults and a more conservative public-facing range of ~18M–26M adults, with a planning midpoint of ~22M adults . This reframes ME/CFS from a rare or niche illness into a mass-scale public health condition and implies that both healthcare and productivity costs are likely far greater than earlier burden models captured.
This pattern reflects a structural issue. ME/CFS is still largely managed using state-agnostic care and trial designs, where interventions are delivered without accounting for biologic state, phenotype variability, or environmental load. Within the Personalized CRISPR Remission™ framework, a meaningful portion of this burden can be understood as recoverable inefficiency driven by misalignment between intervention and terrain.
10.1 Direct Economic Savings (Treatment Efficiency Gains)
Direct savings arise from reducing inefficiencies associated with repeated diagnostics, specialist cycling, ineffective treatment attempts, and escalation of care during periods of biologic instability. Because ME/CFS patients with persistent symptoms often move through multiple providers and repeated management loops, a conservative annual excess direct-care burden can be modeled at approximately $3,000–$7,000 per patient, reflecting repeated diagnostics, medication changes, specialist care, and symptom-management burden under current care patterns (Institute of Medicine, 2015).
For modeling purposes, a midpoint can be used:
Annual excess direct-care burden (ME/CFS) ≈ $5,000 per patient
Applying conservative capture rates based on improved intervention alignment:
25% capture → $1,250 per patient/year
40% capture → $2,000 per patient/year
60% capture → $3,000 per patient/year
These savings reflect:
reduced diagnostic cycling
fewer ineffective interventions
lower adverse-event burden from poorly timed treatment
improved durability of therapeutic response
The logic here is not that every dollar of care disappears, but that a portion of current expenditure represents avoidable variability-driven waste.
10.2 Indirect Economic Value (Productivity and Functional Recovery)
Indirect costs represent a major share of ME/CFS burden because the disease affects work capacity, daily functioning, caregiving demands, and disability dependence over long periods of time. Even under older prevalence assumptions, lost productivity was recognized as one of the largest contributors to total burden (Institute of Medicine, 2015). Given CYNAERA’s corrected prevalence framework, the scale of this burden is almost certainly much larger than older national estimates suggest .
For conservative modeling, a productivity-related burden of approximately $8,000–$15,000 per patient/year can be used, especially in patients with sustained functional impairment, reduced workforce participation, or long-term disability risk.
Using a conservative midpoint:
Estimated productivity-related burden (ME/CFS) ≈ $10,000 per patient/year
Applying modest functional recovery assumptions:
10% functional recovery → $1,000 per patient/year
20% recovery → $2,000 per patient/year
30% recovery → $3,000 per patient/year
These gains reflect:
increased workforce participation
reduced disability dependence
improved daily functioning and reduced caregiver burden
Importantly, these estimates assume partial recovery, not full remission, making them conservative relative to long-term upside.
10.3 Total Economic Value and Scaling Impact
When direct and indirect effects are combined, the value of better-aligned intervention becomes more visible.
Per-patient annual value (conservative range):
Low estimate: ~$2,250 per patient/year
Moderate estimate: ~$4,000 per patient/year
Higher estimate: ~$6,000 per patient/year
At scale, these gains compound rapidly.
For example:
10,000 patients → $22.5M to $60M annual value
100,000 patients → $225M to $600M annual value
1 million patients → $2.25B to $6.0B annual value
Using CYNAERA’s planning midpoint of ~22 million U.S. adults with ME/CFS-classification burden, even modest recovery or efficiency gains imply very large national impact . This is especially relevant because ME/CFS has historically been modeled using prevalence assumptions far below what corrected undercount frameworks now support. These estimates do not include the cost of the CRISPR-based therapeutic itself, which would need to be weighed against long-term savings. However, they show that once ME/CFS is modeled at realistic scale, the economic upside of reducing even a small fraction of chronic inefficiency becomes substantial.
10.4 System-Level Interpretation
The broader implication is structural. In current models, variability is treated as noise, and cost is managed through repeated escalation of care. In a state-dependent framework, variability becomes measurable and actionable. Intervention is aligned with system readiness, reducing inefficiency and improving outcome detection.
This shift reframes CRISPR-based therapies in ME/CFS. They are no longer simply high-cost interventions applied at the far end of a research pipeline. They function as stabilization infrastructure, capable of reducing cumulative system burden, improving trial interpretability, and increasing the proportion of patients who achieve durable improvement. The economic value of advanced therapies is therefore not determined solely by upfront cost, but by their ability to reduce repeated utilization, decrease false-negative trial failure, and restore functional capacity over time.
11. Conclusion: From Static Targeting to State-Dependent Remission
ME/CFS has long been characterized by fragmentation between clinical observation, patient experience, and research design. While substantial progress has been made in identifying abnormalities across immune, metabolic, neurologic, and autonomic systems, these findings have not translated into consistent therapeutic success. As Anthony Komaroff and W. Ian Lipkin have emphasized, the illness is defined not only by its multi-system nature, but by the instability and variability that shape its clinical course (Komaroff and Lipkin, 2021). Without models that account for this variability, even well-supported biologic targets may fail to produce interpretable results.
This paper reframes that challenge as a problem of system alignment rather than data deficiency. By integrating phenotype-stratified classification, state-dependent timing, environmental modeling, and structured stabilization, the Personalized CRISPR Remission™ framework establishes a personalized, customized, and individualized approach to gene editing in ME/CFS. It builds on existing research, including the metabolic insights of Naviaux, the immunologic work of Hanson, and the systems modeling approaches advanced by Klimas and colleagues, while addressing the gap between these findings and their application in clinical trials (Naviaux et al., 2016; Hanson et al., 2016; Klimas et al., 2012).
A central implication of this work is that intervention success in ME/CFS cannot be evaluated independently of the conditions under which it is delivered. Phenotypic heterogeneity, environmental exposure, autonomic stability, and metabolic capacity are not peripheral considerations. They are determinants of whether a given intervention can be tolerated, interpreted, and sustained. Frameworks such as VitalGuard™ and the Terrain Response Score (TRS), developed within CYNAERA’s Microdosing Air™ model, extend this logic by demonstrating that environmental variables can be both predictive and modifiable, allowing state-dependent gene-editing interventions to be aligned with periods of reduced system load.
This perspective also clarifies the role of patient behavior within the disease model. The strategies patients use to manage pacing, exposure, and physiologic stress are not simply coping mechanisms. They represent an unmodeled layer of system intelligence that reflects the underlying dynamics of the disease. Incorporating this knowledge into formal research design bridges a long-standing gap between lived experience and clinical investigation, transforming patient-informed strategies into structured components of customized and individualized intervention design. The implications for clinical trial design are substantial. Trials that incorporate phenotype stratification, state-dependent timing, and environmental alignment are more likely to detect meaningful signals, reduce variability, and produce results that reflect true biologic effects. By contrast, approaches that continue to rely on static models risk perpetuating the cycle of inconclusive findings that has defined the field to date.
The Personalized CRISPR Remission™ framework does not assume that gene editing alone will resolve ME/CFS. Rather, it provides a structure within which personalized gene editing, precision CRISPR-based interventions, and related advanced biologic strategies, including CAR-T and other immune-engineered therapies, can be evaluated under conditions that reflect the complexity of the disease. In doing so, it shifts the field from isolated intervention toward coordinated system design, where phenotype, timing, environment, and stabilization are treated as integral components of therapeutic success.
In ME/CFS, clinical trial outcomes are not determined solely by the intervention itself, but by whether the system in which that intervention is delivered has been properly defined, stabilized, and aligned. When that alignment is achieved, variability becomes interpretable, therapeutic signal becomes detectable, and state-dependent, personalized gene-editing strategies move closer to enabling durable remission and, ultimately, cure.
This model is further supported by The Eve Research Project, an ongoing research program designed to capture real-world disease trajectories across immune activity, hormonal transitions, and environmental stressors. These insights are critical for identifying when patients are biologically stable enough for advanced interventions and when underlying instability may increase risk.
This work is, in part, a recognition of the patients who held on through years of severe illness, isolation, and loss while the field failed to build models that matched the reality of their disease. Many of the principles formalized here were first learned through survival. They were carried by patients who continued to observe, adapt, and endure even when ME/CFS had stripped away function, certainty, and much of ordinary life.
Frequently Asked Questions
Is CRISPR Remission™ intended to cure ME/CFS?
Yes, the long-term ambition of CRISPR Remission™ is to support cure-level intervention in ME/CFS. However, the framework does not assume that first-generation applications will produce immediate or universal cure. Its current purpose is to make remission-oriented gene editing safer, more interpretable, and more durable by aligning targets with biologic state, phenotype, and system readiness.
Why does timing matter so much in ME/CFS?
Because ME/CFS is a state-dependent condition characterized by fluctuating immune, metabolic, and autonomic function. The same intervention can produce different outcomes depending on when it is applied relative to system stability (Chu et al., 2019).
How is this different from personalized medicine?
Personalized medicine typically adjusts treatment based on patient characteristics. Personalized CRISPR Remission™ goes further by incorporating dynamic system state, meaning treatment is adapted not only to the patient, but to their condition at a specific moment in time.
Why emphasize stabilization before intervention?
Because unstable systems cannot reliably process therapeutic input. Stabilization reduces variability, improves tolerability, and increases the likelihood that intervention effects can be detected and sustained.
Does this replace existing ME/CFS research approaches?
No. It integrates with them. The framework connects phenotyping, genomics, environmental modeling, and clinical design into a unified system rather than treating them as separate domains.
Can this framework apply beyond ME/CFS?
Yes. Although this paper focuses on ME/CFS, Personalized CRISPR Remission™ is designed as a broader platform for autoimmune disease, immune-volatile cancer states, Long COVID, dysautonomia, POTS, mast cell activation syndrome, Lyme disease, post-treatment Lyme disease syndrome, fibromyalgia, and related neuroimmune or infection-associated chronic conditions. The core principle remains the same across these illnesses: intervention success depends on system state, biologic timing, and terrain readiness rather than diagnosis alone.
Appendices
Appendix A. Expanded Candidate Gene Modeling for ME/CFS
This appendix defines the broader gene-target landscape underlying CYNAERA’s Personalized CRISPR Remission™ framework for ME/CFS. Rather than presenting isolated targets, this model reflects a state-dependent, multi-domain system in which gene selection, intervention timing, and physiologic readiness must be aligned. Broader modeling within CYNAERA’s architecture constrains the ME/CFS intervention landscape to approximately 118 prioritized genes spanning immune regulation, metabolic function, autonomic signaling, neuroinflammation, and environmental response pathways. This set represents a dynamic modeling universe, not a fixed therapeutic panel, and is refined continuously based on phenotype-specific and state-dependent evidence.
A1. Domain Structure of the 118-Gene Model
Domain | Functional Role | Approx. Gene Allocation |
Neuroimmune and Neuroinflammatory | Cytokine signaling, microglial activation, synaptic and neuroimmune regulation | ~25 |
Metabolic and Mitochondrial | Energy production, oxidative stress, cellular recovery capacity | ~20 |
Autonomic and Cardiovascular | Adrenergic signaling, vascular tone, endothelial and circulatory regulation | ~15 |
Immune Regulation and Viral Persistence | NK function, checkpoint pathways, viral latency and chronic immune activation | ~30 |
Environmental Response and Hypersensitivity | Detoxification, mast cell signaling, exposure-triggered inflammatory response | ~28 |
Total modeled targets: approximately 118 genes
A2. Representative Structure of the 118-Gene Model
Domain | Mechanism Cluster | Representative Genes | Primary Mechanisms Impacted |
Neuroimmune and Neuroinflammatory | Pro-inflammatory cytokine signaling | IL1B, IL6, TNF, IFNG | Inflammatory amplification, fatigue signaling, neuroimmune stress |
Neuroimmune and Neuroinflammatory | Inflammasome and innate activation | NLRP3, TLR4, P2RX7 | Danger sensing, cytokine release, innate immune escalation |
Neuroimmune and Neuroinflammatory | Cytokine transduction and immune feedback | STAT1, STAT3, JAK1, JAK2, SOCS3 | Signal relay, inflammatory persistence, negative feedback control |
Neuroimmune and Neuroinflammatory | Chemokine trafficking and antigen presentation | CCL2, CCL5, CCR5, HLA-DRA, HLA-DRB1 | Immune cell recruitment, antigen presentation, chronic inflammation |
Neuroimmune and Neuroinflammatory | Synaptic and neuroregulatory signaling | BDNF, SYNGAP1, GRIN2A, SLC6A4, COMT, NOS1, GSK3B | Cognitive processing, excitatory balance, catecholamine handling, neurovascular signaling |
Metabolic and Mitochondrial | NAD and energy-sensing pathways | NAMPT, PRKAA1, PRKAA2, SIRT1, SIRT3, mTOR | NAD biosynthesis, AMPK signaling, metabolic adaptation, nutrient sensing |
Metabolic and Mitochondrial | Mitochondrial biogenesis and respiration | PPARGC1A, TFAM, ATP5F1A, COX4I1, UQCRC1, UCP2 | Mitochondrial output, oxidative phosphorylation, respiratory efficiency |
Metabolic and Mitochondrial | Pyruvate and metabolic switching | PDHA1, PDK4, LDHA, HIF1A | Glucose oxidation, anaerobic metabolism, hypoxia adaptation |
Metabolic and Mitochondrial | Oxidative stress and redox defense | NFE2L2, SOD2, GPX1, CAT | Antioxidant response, redox stability, oxidative damage control |
Autonomic and Cardiovascular | Adrenergic regulation | ADRB1, ADRB2, ADRA1A, ADRA2A, TH, DBH | Sympathetic tone, catecholamine signaling, autonomic balance |
Autonomic and Cardiovascular | RAAS and vascular response | ACE, ACE2, AGT, AGTR1 | Blood pressure regulation, circulatory stability, vascular-autonomic tone |
Autonomic and Cardiovascular | Endothelial and vascular integrity | NOS3, EDN1, VEGFA, GCH1, SCN10A | Endothelial function, vasoconstriction, perfusion, autonomic conduction |
Immune Regulation and Viral Persistence | Checkpoint and exhaustion pathways | PDCD1, CD274, CTLA4, LAG3, TIGIT | Immune restraint, T-cell exhaustion, chronic activation control |
Immune Regulation and Viral Persistence | NK and cytotoxic function | NCR1, KLRK1, PRF1, GZMB | Cytotoxic surveillance, immune clearance, NK cell function |
Immune Regulation and Viral Persistence | Interferon and antiviral defense | IFITM3, IRF7, MX1, OAS1, RNASEL, STAT2, DDX58, MAVS, TRIM25 | Antiviral sensing, interferon signaling, viral restriction |
Immune Regulation and Viral Persistence | Chemokine and tolerance regulation | CXCL9, CXCL10, IL10, TGFB1, FOXP3, B2M, TAP1 | Immune recruitment, immune braking, tolerance, antigen processing |
Immune Regulation and Viral Persistence | Stress response and viral persistence context | HSPA1A, XBP1, EIF2AK3, EBNA1-related host genes, LMP1-related host genes | ER stress, protein response, viral latency, immune evasion context |
Environmental Response and Hypersensitivity | Mast cell and histamine signaling | KIT, TPSAB1, HDC, HRH1, HRH2, MRGPRX2 | Mast cell activation, histamine signaling, hypersensitivity response |
Environmental Response and Hypersensitivity | Th2 and alarmin biology | FCER1A, IL4, IL13, IL33, TSLP | Allergic skewing, epithelial alarm signaling, hypersensitivity amplification |
Environmental Response and Hypersensitivity | Pollutant sensing and detoxification | AHR, CYP1A1, CYP1B1, GSTM1, GSTT1, NQO1, ALDH2, HMOX1 | Xenobiotic sensing, detoxification, oxidative stress buffering |
Environmental Response and Hypersensitivity | Sensory and irritant signaling | TRPA1, TRPV1 | Chemical irritant sensing, neurogenic inflammation, sensory hypersensitivity |
Environmental Response and Hypersensitivity | Barrier and mucosal integrity | CLDN1, OCLN, AQP5, MUC1, MUC5B, SERPINB2, SOD1 | Tight junction function, mucosal defense, epithelial resilience, inflammatory buffering |
Where These ME/CFS-Relevant Targets Have Already Been Edited in Other Conditions
Several of the gene targets relevant to ME/CFS have already been edited in other disease areas, even if they have not yet been pursued in ME/CFS itself. This matters because it shows that parts of the biological terrain you are mapping are not speculative in a gene-editing sense. What is novel in CYNAERA’s framing is not simply the target list, but the state-dependent logic for when those targets may become viable in an unstable, multi-system illness environment.
PDCD1 (PD-1) has already been edited in primary human T cells and in engineered anti-tumor T-cell settings. One early study used CRISPR-Cas9 to disrupt PD-1 in human primary T cells, while later clinical and translational work advanced PD-1-disrupted engineered T cells in cancer settings, including refractory solid tumors and CAR-T platforms (Su et al., 2016; Wang et al., 2021; Stadtmauer et al., 2020).
CTLA4 has also already been edited in other conditions. Therapeutic gene editing has been used to correct CTLA4 insufficiency in patient T cells, and preclinical immunotherapy work has used CTLA4 deletion to enhance engineered T-cell function, particularly in cancer contexts (Fox et al., 2022; Agarwal et al., 2023).
KIT has some of the clearest precedent for the mast cell and MCAS-overlap side of the framework. CRISPR/Cas9 has been used to reverse a KIT mutation in HMC-1.2 mast cells, creating a more refined mastocytosis model, and related studies have continued to use KIT-edited mast cell systems to study disease biology and intervention logic (Bandara et al., 2023; Snider et al., 2021).
PPARGC1A has already been directly activated with CRISPRa in mitochondrial and cardiometabolic contexts. A recent study showed that CRISPR-based activation of PPARGC1A increased mitochondrial content and improved function, supporting the idea that mitochondrial biogenesis targets can be manipulated in living disease systems rather than only discussed theoretically (Escobar et al., 2026).
For the autonomic and vascular cluster, the best direct precedent is within the RAAS pathway, even if not always at the exact same node you would prioritize in ME/CFS. CRISPR-Cas9 deletion of hepatic angiotensinogen has already been used in preclinical hypertension work and produced sustained blood pressure reduction, which supports the broader claim that RAAS biology has already been gene-edited in cardiovascular disease contexts (Sun et al., 2021).
NLRP3 has been directly targeted with CRISPR/Cas9 in inflammatory disease models. One notable study used nanoparticle-delivered CRISPR/Cas9 to inactivate NLRP3 in macrophages and showed anti-inflammatory effects in vivo, making this one of the stronger examples of direct editing precedent for inflammatory signaling rather than merely pathway association (Xu et al., 2018).
CX3CR1 has mainly been edited in neuroimmune and microglial model systems. Human induced pluripotent stem cell-derived microglia have been engineered with CRISPR/Cas9 to disrupt CX3CR1 in order to study phagocytosis, inflammatory response, and homeostatic regulation. That makes this a meaningful precedent target for neuroimmune modeling, though not yet a mature clinical deployment example (Nobohito et al., 2020).
AHR also has documented CRISPR precedent, though it is more mechanistic than clinically translated. CRISPR-Cas9 knockout approaches have been used to study AHR function in environmental response, epithelial biology, toxicology, and tumor-regulatory signaling, which supports its relevance as an environmental sensitivity target while also showing that the translational maturity here is still earlier than for targets like PDCD1 or KIT (Liebert et al., 2023; Fu et al., 2023; Zhang et al., 2025).
Some of the other genes in the ME/CFS phenotype-target-timing framework, including adrenergic receptor targets, TPSAB1, OAS1, IFITM3, IRF7, PRF1, and NCR1, are still better framed as biologically relevant candidate or subgroup targets than as strongly established edited targets in other diseases. In those cases, the literature is currently stronger for pathway relevance, immune function, or disease modeling than for mature intervention precedent.
Appendix B: Phenotype–Target–Timing Alignment (State-Dependent Model)
Phenotype Domain | Dominant System Features | Primary Target Clusters | Intervention Timing Logic |
Neuroimmune / Cognitive | Brain fog, neuroinflammation, sensory overload, cognitive PEM | Cytokine signaling (IL1B, IL6, TNF), inflammasome (NLRP3), microglial signaling (CX3CR1), synaptic regulation (BDNF, GRIN2A) | Avoid active PEM or neuroinflammatory spikes. Intervene during low sensory load and reduced cytokine activity. |
Metabolic / PEM-Dominant | Severe post-exertional malaise, low energy reserve, delayed recovery | NAD and AMPK pathways (NAMPT, PRKAA1/2), mitochondrial biogenesis (PPARGC1A, TFAM), oxidative stress (NFE2L2, SOD2) | Strictly avoid post-exertional states. Requires stable baseline energy and preserved metabolic capacity prior to intervention. |
Autonomic / POTS-Dominant | Tachycardia, orthostatic intolerance, vascular instability | Adrenergic signaling (ADRB1/2, ADRA1A/2A), RAAS (ACE, AGTR1), endothelial function (NOS3, VEGFA) | Align with cardiovascular stability. Avoid dehydration, heat, travel, and orthostatic stress periods. |
Immune Activation / Viral Reactivation | EBV/HHV-6 patterns, low NK function, chronic immune activation | Checkpoint pathways (PDCD1, CTLA4), NK function (NCR1, PRF1), antiviral signaling (OAS1, IFITM3, IRF7) | Avoid periods of acute immune activation. Intervene during controlled, stabilized immune states. |
Environmental Sensitivity / MCAS-Overlap | Chemical sensitivity, mold-triggered flares, histamine reactivity | Mast cell signaling (KIT, TPSAB1), histamine pathways (HRH1/2), detox and pollutant response (AHR, CYP1A1, GSTM1) | Requires low environmental load. Must align with controlled air quality, low allergen exposure, and minimal cumulative exposure burden. |
Multi-System / High Variability | Cross-domain instability, frequent crashes, high symptom volatility | Multi-domain clusters across immune, metabolic, autonomic, and environmental pathways | Intervention often deferred. Requires full stabilization (STAIR) and narrow readiness window before any gene-target engagement. |
CRISPR success in ME/CFS is not phenotype-dependent alone. It is phenotype + timing + system state dependent.
Appendix C: Phenotype-Stratified Clinical Trial Architecture (ME/CFS)
Within the Personalized CRISPR Remission™ framework, clinical trial design shifts from diagnosis-based enrollment to phenotype- and state-aligned cohort structuring. Rather than evaluating a single intervention across a heterogeneous population, participants are stratified into biologically coherent groups based on dominant system involvement and current terrain conditions. This allows intervention effects to be evaluated within aligned physiologic contexts, reducing signal dilution and improving interpretability.
Trial Structure Overview
Participants are assigned to arms based on dominant phenotype cluster, with each arm incorporating:
phenotype-specific target selection
state-dependent timing criteria
pre-intervention stabilization requirements
environmental alignment protocols (VitalGuard™)
Each arm operates as a semi-independent cohort, allowing for both within-arm signal detection and cross-arm comparison.
Trial Arms
Arm A: Immune-Dominant Cohort
Inclusion Profile:
Elevated inflammatory markers or cytokine activity
Post-viral onset or reactivation patterns
Immune-triggered flares
Primary Targets:
IL12A
STAT signaling pathways
TNF / IL-6 modulation
Pre-Intervention Requirements:
No active flare or infection
Stabilized inflammatory markers (relative baseline)
Timing Logic:
Intervention scheduled during low-inflammatory windows
VitalGuard™ used to avoid high-exposure or immune-activating periods
Outcome Focus:
Reduction in flare frequency
Improved immune stability
Decreased symptom volatility
Arm B: Metabolic-Dominant Cohort
Inclusion Profile:
Severe PEM
Low energy reserve
mitochondrial dysfunction patterns
Primary Targets:
NAMPT
SIRT pathways
AMPK regulation
Pre-Intervention Requirements:
No recent PEM episode (minimum stabilization window)
preserved baseline function
Timing Logic:
Intervention during energy-stable periods only
strict avoidance of post-exertional states
Outcome Focus:
Improved exertion tolerance
reduced PEM severity
increased baseline energy capacity
Arm C: Autonomic-Dominant Cohort
Inclusion Profile:
POTS or orthostatic intolerance
vascular instability
dysregulated heart rate or blood pressure
Primary Targets:
ACE / RAAS pathways
adrenergic signaling pathways
endothelial regulation
Pre-Intervention Requirements:
hydration optimized
medication stabilized (beta blockers, etc.)
Timing Logic:
Avoid heat, travel, and dehydration periods
align with stable cardiovascular states
Outcome Focus:
improved orthostatic tolerance
reduced tachycardia variability
improved circulatory stability
Arm D: Neuroimmune / Cognitive Cohort
Inclusion Profile:
brain fog
neuroinflammation
sensory sensitivity
Primary Targets:
neuroinflammatory pathways
microglial activation
excitatory signaling regulation
Pre-Intervention Requirements:
reduced sensory load
stabilized sleep and cognitive baseline
Timing Logic:
avoid high cognitive demand periods
align with low neuroinflammatory states
Outcome Focus:
improved cognitive clarity
reduced sensory overload
improved processing stability
Arm E: Multi-System / High-Instability Cohort
Inclusion Profile:
cross-axis involvement
frequent crashes
high variability
Primary Targets:
staged or combination approach
stabilization pathways prioritized
Pre-Intervention Requirements:
full STAIR: Stable Method™ protocol
environmental and physiologic stabilization
Timing Logic:
intervention only during narrow stability windows
may require delayed entry into active intervention phase
Outcome Focus:
reduced system volatility
improved baseline stability
expanded intervention tolerance
Cross-Arm System Controls
All arms incorporate:
1. State-Dependent Timing
interventions scheduled based on biologic readiness, not calendar timing
2. Environmental Alignment (VitalGuard™)
avoid high-risk windows (pollution, storms, heat, mold spikes)
identify optimal 48–72 hour intervention windows
3. Pre-Intervention Stabilization
STAIR: Stable Method™ protocols
pacing, hydration, medication alignment
environmental exposure control
4. Dynamic Monitoring
SymCas™ for flare prediction
real-time adjustment of intervention timing
Why This Trial Design Works
Traditional ME/CFS trials fail because they:
group heterogeneous patients together
ignore state variability
apply interventions at arbitrary time points
fail to control environmental confounders
This model corrects those issues by:
aligning cohorts with biology
aligning timing with system state
controlling environmental variability
preserving signal integrity
CYNAERA Framework Papers and Core Research Libraries
This paper draws on a defined subset of CYNAERA Institute white papers that establish the methodological and analytical foundations of CYNAERA’s frameworks. These publications provide deeper context on prevalence reconstruction, remission, combination therapies and biomarker approaches. Our Long COVID Library, ME/CFS Library, Lyme Library, Autoimmune Library and CRISPR Remission Library are also in depth resources.
Author’s Note:
All insights, frameworks, and recommendations in this written material reflect the author's independent analysis and synthesis. References to researchers, clinicians, and advocacy organizations acknowledge their contributions to the field but do not imply endorsement of the specific frameworks, conclusions, or policy models proposed herein. This information is not medical guidance.
Patent-Pending Systems
Bioadaptive Systems Therapeutics™ (BST) and affiliated CYNAERA frameworks are protected under U.S. Provisional Patent Application No. 63/909,951. CYNAERA is built as modular intelligence infrastructure designed for licensing, integration, and strategic deployment across health, research, public sector, and enterprise environments.
Licensing and Integration
CYNAERA supports licensing of individual modules, bundled systems, and broader architecture layers. Current applications include research modernization, trial stabilization, diagnostic innovation, environmental forecasting, and population level modeling for complex chronic conditions. Basic licensing is available through CYNAERA Market, with additional pathways for pilot programs, institutional partnerships, and enterprise integration.
About the Author
Cynthia Adinig is the founder of CYNAERA, a modular intelligence infrastructure company that transforms fragmented real world data into predictive insight across healthcare, climate, and public sector risk environments. Her work sits at the intersection of AI infrastructure, federal policy, and complex health system modeling, with a focus on helping institutions detect hidden costs, anticipate service demand, and strengthen planning in high uncertainty environments.
Cynthia has contributed to federal health and data modernization efforts spanning HHS, NIH, CDC, FDA, AHRQ, and NASEM, and has worked with congressional offices including Senator Tim Kaine, Senator Ed Markey, Representative Don Beyer, and Representative Jack Bergman on legislative initiatives related to chronic illness surveillance, healthcare access, and data infrastructure. In 2025, she was appointed to advise the U.S. Department of Health and Human Services and has testified before Congress on healthcare data gaps and system level risk.
She is a PCORI Merit Reviewer, currently advises Selin Lab at UMass Chan, and has co-authored research with Harlan Krumholz, MD, Akiko Iwasaki, PhD, and David Putrino, PhD, including through Yale’s LISTEN Study. She also advised Amy Proal, PhD’s research group at Mount Sinai through its CoRE advisory board and has worked with Dr. Peter Rowe of Johns Hopkins on national education and outreach focused on post-viral and autonomic illness. Her CRISPR Remission™ abstract was presented at CRISPRMED26 and she has authored a Milken Institute essay on artificial intelligence and healthcare.
Cynthia has been covered by outlets including TIME, Bloomberg, Fortune, and USA Today for her policy, advocacy, and public health work. Her perspective on complex chronic conditions is also informed by lived experience, which sharpened her commitment to reforming how chronic illness is understood, studied, and treated. She also advocates for domestic violence prevention and patient safety, bringing a trauma informed lens to her research, systems design, and policy work. Based in Northern Virginia, she brings more than a decade of experience in strategy, narrative design, and systems thinking to the development of cross sector intelligence infrastructure designed to reduce uncertainty, improve resilience, and support institutional decision making at scale.
References
Afrin, L. B., Weinstock, L. B., and Molderings, G. J. (2020). Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome. International Journal of Infectious Diseases, 100, 327–332.
Akdis, C. A., and Akdis, M. (2011). Mechanisms of allergen-specific immunotherapy. Journal of Allergy and Clinical Immunology, 127(1), 18–27.
Bateman, L., Bested, A. C., Bonilla, H. F., et al. (2021). Myalgic encephalomyelitis/chronic fatigue syndrome: Essentials of diagnosis and management. Mayo Clinic Proceedings, 96(11), 2861–2878.
Boström, C. E., Gerde, P., Hanberg, A., et al. (2002). Cancer risk assessment, indicators, and guidelines for polycyclic aromatic hydrocarbons in ambient air. Environmental Health Perspectives, 110(Suppl 3), 451–488.
Castells, M. (2017). Diagnosis and management of anaphylaxis in precision medicine. Journal of Allergy and Clinical Immunology, 140(2), 321–333.
Chen, P. J., Hussmann, J. A., Yan, J., et al. (2024). Enhanced prime editing systems for improved precision gene editing. Nature Biotechnology.
Chu, L., Valencia, I. J., Garvert, D. W., and Montoya, J. G. (2019). Onset patterns and course of myalgic encephalomyelitis/chronic fatigue syndrome. Frontiers in Pediatrics, 7, 12.
Ciencewicki, J., and Jaspers, I. (2007). Air pollution and respiratory viral infection. Inhalation Toxicology, 19(14), 1135–1146.
Dominici, F., Peng, R. D., Bell, M. L., et al. (2006). Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA, 295(10), 1127–1134.
Doudna, J. A. (2020). The promise and challenge of therapeutic genome editing. Nature, 578, 229–236.
Doudna, J. A., and Charpentier, E. (2014). The new frontier of genome engineering with CRISPR-Cas9. Science, 346(6213).
Drzazga, A., Rola, R., and Wójcik, M. (2021). Volatile organic compounds and their impact on human health. Environmental Research.
Durham, S. R., and Shamji, M. H. (2019). Allergen immunotherapy: Past, present and future. Nature Reviews Immunology, 19(12), 761–773.
Fisk, W. J., Eliseeva, E. A., and Mendell, M. J. (2010). Association of residential dampness and mold with respiratory tract infections and bronchitis. Environmental Health, 9, 72.
Fluge, Ø., and Mella, O. (2019). Clinical trials of B-cell depletion therapy in ME/CFS. Annals of Internal Medicine.
Gawda, A., Majka, G., Nowak, B., and Marcinkiewicz, J. (2018). Air pollution, oxidative stress, and inflammation. Advances in Experimental Medicine and Biology.
Goldstein, D. S. (2020). The extended autonomic system, dyshomeostasis, and COVID-19. Clinical Autonomic Research.
Habib, O., Habib, G., and Hossain, M. (2023). Lipid nanoparticle delivery systems for gene editing. Molecular Therapy.
Hanna, R., Dweik, R., and others (2021). VOC exposure and respiratory and systemic inflammation. Journal of Clinical Medicine.
Hanson, M. R., et al. (2016). Metabolic and immune alterations in ME/CFS. Proceedings of the National Academy of Sciences.
Hollingsworth, J. W., et al. (2007). Ozone and pulmonary inflammation. American Journal of Respiratory Cell and Molecular Biology.
Institute of Medicine (2015). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. National Academies Press.
Jason, L. A., et al. (2011). Energy envelope theory and symptom patterns in ME/CFS. Journal of Human Behavior in the Social Environment.
Jason, L. A., et al. (2013). Self-management and coping strategies in ME/CFS. Health Care for Women International.
Ji, R. R., et al. (2018). Neuroinflammation and central sensitization. Nature Reviews Neuroscience.
Kim, K. H., Jahan, S. A., and Kabir, E. (2013). Polycyclic aromatic hydrocarbons and human health. Environment International.
Klaassen, K., et al. (2025). Genomic insights into ME/CFS. Emerging Infectious Diseases / Preprint.
Komaroff, A. L., and Lipkin, W. I. (2021). ME/CFS pathophysiology and immune dysfunction. Nature Reviews Disease Primers.
Klimas, N. G., et al. (2012). Systems biology approaches to ME/CFS. Pharmacogenomics.
Lee, J. S., Sato, W., and Son, C. G. (2023). Neuroinflammation and network dysfunction in ME/CFS. Journal of Translational Medicine.
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation. Physiological Reviews.
Mukamal, K. J., et al. (2009). Weather and cardiovascular events. Circulation.
Naldini, L. (2015). Gene therapy returns to centre stage. Nature.
National Academies of Sciences (2015). ME/CFS diagnostic and biological framework.
Natelson, B. H., et al. (2021). Brain and autonomic dysfunction in ME/CFS. Frontiers in Neurology.
Naviaux, R. K., et al. (2016). Metabolic features of ME/CFS. Proceedings of the National Academy of Sciences.
Pardi, N., Hogan, M. J., Porter, F. W., and Weissman, D. (2018). mRNA vaccines and delivery systems. Nature Reviews Drug Discovery.
Park, J. H., et al. (2006). Dampness and indoor environmental quality. Environmental Health Perspectives.
Pope, C. A., et al. (2016). Air pollution and cardiovascular disease. Circulation Research.
Raj, S. R., et al. (2021). Postural orthostatic tachycardia syndrome. Circulation.
Shan, Z. Y., et al. (2020). Brain connectivity abnormalities in ME/CFS. NeuroImage: Clinical.
Sterling, P. (2012). Allostasis and predictive regulation. Physiology & Behavior.
Valent, P., et al. (2019). Mast cell activation syndromes. Journal of Allergy and Clinical Immunology.
VanElzakker, M. B., et al. (2019). Neuroinflammation in ME/CFS. Psychopharmacology.
Vertigan, A. E., et al. (2016). Weather and respiratory/autonomic symptoms. Journal of Thoracic Disease.
Walitt, B., et al. (2024). ME/CFS symptom variability and trajectory. NIH / Preprint.
Weinstock, L. B., et al. (2021). Mast cell activation and systemic illness. Annals of Allergy.
Wiborg, J. F., et al. (2023). Genetic and molecular markers in ME/CFS. Translational Psychiatry.
Wong, T. L., et al. (2023). Health disparities in chronic illness. Health Equity.
World Health Organization (2022). Air Quality Guidelines.



Comments