
CDF-Lupus™: Composite Diagnostic Fingerprint For Lupus
- Apr 25
- 10 min read
Updated: May 12
A Multi-System Framework for High-Specificity Diagnosis
By Cynthia Adinig
This paper is part of the CYNAERA Autoimmune Library, a systems-based resource modeling autoimmune disease across multi-domain terrain to improve diagnosis, predict flares, and guide personalized pathways to remission.
Introduction: Why Lupus Is Still Being Missed
Systemic lupus erythematosus (SLE) is widely recognized as a complex autoimmune disease, yet it remains one of the most difficult conditions to diagnose accurately and early. While classification criteria have improved over time, real-world diagnosis still relies on fragmented clinical interpretation across multiple specialties. Patients frequently present with symptoms that evolve over time and span multiple organ systems, making early recognition inconsistent and delayed (Fanouriakis et al., 2019; Aringer et al., 2019; Bertsias et al., 2012).
In practice, lupus behaves as a dynamic, multi-system condition shaped by immune dysregulation, genetic susceptibility, environmental triggers, and hormonal influences (Tsokos, 2011; Kaul et al., 2016; Lisnevskaia et al., 2014). Symptoms rarely appear all at once. Instead, they accumulate, fluctuate, and migrate across systems, often leading to years of partial diagnoses before full classification is reached (Yazdany and Schmajuk, 2014).
Patients are often evaluated in silos, with joint pain sent to rheumatology, rashes to dermatology, fatigue dismissed, and neurological symptoms treated separately. The result is not a lack of disease, but a failure to recognize the pattern (Mosca et al., 2010). CDF-Lupus™ was developed to address this gap by translating systemic autoimmune disease into a structured, multi-domain diagnostic model that reflects how lupus actually presents in patients.
What Is CDF-Lupus™?
CDF-Lupus™ is a composite diagnostic framework that evaluates lupus through cross-system pattern recognition rather than strict reliance on classification criteria alone. Instead of asking whether a patient meets a fixed number of criteria at a single point in time, the model assesses how strongly their presentation aligns with a broader lupus-associated disease pattern across multiple domains.
The framework organizes disease expression across interacting systems, including immune activation, organ involvement, neuroimmune signaling, metabolic disruption, and environmental triggers. This reflects the known heterogeneity of lupus, where disease manifestations vary widely between patients and across time (Tsokos, 2011; Kaul et al., 2016; Rahman and Isenberg, 2008).
CDF-Lupus™ translates these domains into a quantifiable diagnostic fingerprint. Each domain contributes weighted evidence based on signal strength, reliability, specificity, and contextual modifiers such as flare patterns or environmental exposures. Importantly, this model does not replace existing classification systems such as ACR or EULAR criteria. It complements them by identifying disease patterns earlier and more consistently (Aringer et al., 2019; Fanouriakis et al., 2019).
The Core Problem: Lupus as a Pattern Recognition Failure
Lupus is frequently delayed in diagnosis not because it is rare, but because its presentation is temporally and systemically distributed (Lisnevskaia et al., 2014).
Patients often present with:
fatigue and systemic inflammation
joint pain and musculoskeletal symptoms
dermatologic manifestations (malar rash, photosensitivity)
neurological symptoms including brain fog or headaches
cardiovascular or renal involvement
hematologic abnormalities
These features often emerge over time rather than simultaneously. Classification criteria require accumulation of findings, which means early disease is frequently missed (Aringer et al., 2019; Bertsias et al., 2012).
Even when laboratory markers such as ANA are positive, they lack specificity and must be interpreted within a broader clinical context (Pisetsky et al., 2018). Without a structured model, early signals are dismissed or treated in isolation. At a biological level, lupus reflects a breakdown in both innate and adaptive immune regulation, with key contributions from type I interferon signaling, autoreactive B-cell expansion, immune complex deposition, and dysregulated T-cell responses that drive chronic inflammation and tissue damage (Tsokos, 2011; Crow, 2014; Kaul et al., 2016). CDF-Lupus™ resolves this by converting distributed signals into a unified diagnostic structure.
CDF-Lupus™ Domain Architecture
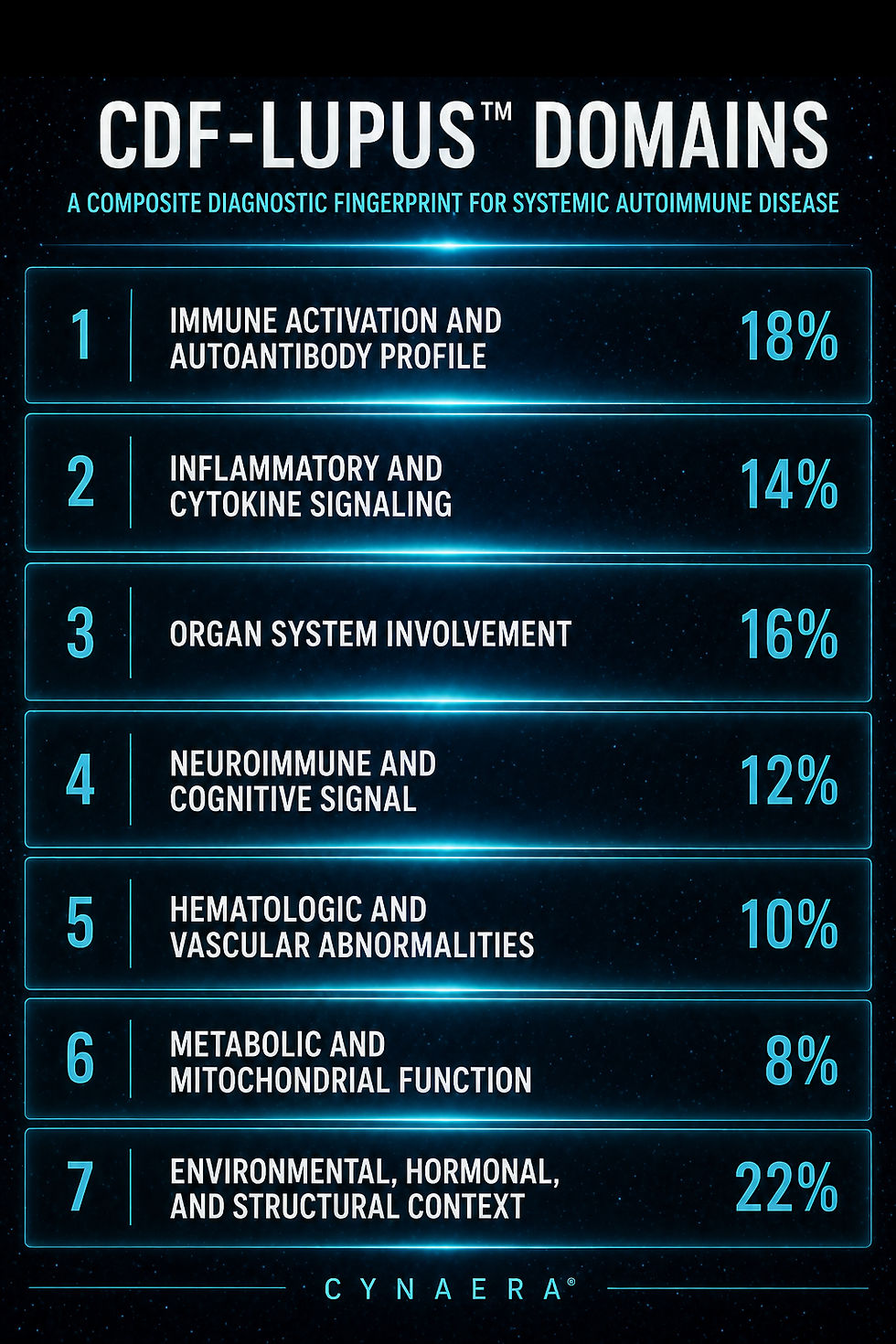
The CDF-Lupus™ framework organizes systemic autoimmune disease into a structured domain architecture adapted from CYNAERA’s multi-condition diagnostic modeling systems. Each domain captures a distinct layer of disease expression, from immune activation and organ involvement to neurocognitive signaling and environmental context. This architecture enables consistent evaluation across heterogeneous lupus presentations by weighting both biological and systemic contributors to disease recognition. The model incorporates the following domains and weights:
Core Domain Structure
Domain 1. Immune Activation and Autoantibody Profile (18%)
Captures core autoimmune signaling, including ANA, anti-dsDNA, anti-Smith antibodies, and broader autoreactive B-cell activity. Lupus is fundamentally driven by loss of immune tolerance, with autoantibody production serving as a central but not standalone diagnostic signal (Rahman and Isenberg, 2008; Tsokos, 2011).
Domain 2. Inflammatory and Cytokine Signaling (14%)
Represents systemic inflammatory activity, including cytokine cascades and type I interferon signaling. Lupus is characterized by persistent immune activation that drives tissue damage and symptom variability across disease states (Crow, 2014; Kaul et al., 2016).
Domain 3. Organ System Involvement (16%)
Measures multi-organ impact, including renal (lupus nephritis), dermatologic (malar rash, photosensitivity), musculoskeletal, and cardiopulmonary involvement. Organ-specific manifestations are often the defining features that move patients toward formal classification (Fanouriakis et al., 2019).
Domain 4. Neuroimmune and Cognitive Signal (12%)
Captures neurological and cognitive involvement, including brain fog, headaches, mood changes, and neuroinflammatory symptoms. Neuroimmune disruption is frequently underrecognized in lupus despite its impact on function and quality of life (Hanly et al., 2010).
Domain 5. Hematologic and Vascular Abnormalities (10%)
Assesses blood and vascular involvement, including anemia, leukopenia, thrombocytopenia, and clotting abnormalities such as antiphospholipid activity. These features reflect systemic immune dysfunction extending into circulation and vascular integrity (Cervera et al., 2009).
Domain 6. Metabolic and Mitochondrial Function (8%)
Evaluates energy metabolism, mitochondrial efficiency, and systemic fatigue patterns. While not traditionally emphasized in lupus criteria, metabolic dysfunction contributes significantly to disease burden and functional decline (Perl, 2013).
Domain 7. Environmental, Hormonal, and Structural Context (22%)
Captures external and systemic modifiers of disease expression, including UV exposure, infections, hormonal fluctuations, stress, and structural barriers to care such as delayed diagnosis and fragmented specialty access. Lupus is highly sensitive to environmental and hormonal triggers, and this domain reflects both biologic reactivity and real-world diagnostic friction (Lisnevskaia et al., 2014; Yazdany and Schmajuk, 2014).
These domains reflect lupus as a dynamic, multi-system condition rather than a static checklist-based disease. The distribution of weights emphasizes that while immune activation is central, environmental context, hormonal modulation, and systemic pattern recognition play an equally critical role in how lupus presents and is ultimately diagnosed.
The strong weighting of environmental, hormonal, and structural context highlights a core CYNAERA principle: diagnostic delay in lupus is not solely a failure of biology, but a failure of systems to recognize distributed signals across time (Aringer et al., 2019; Fanouriakis et al., 2019; Yazdany and Schmajuk, 2014). Underlying disease mechanisms involve dysregulated innate and adaptive immunity, including interferon pathway activation, autoreactive B-cell expansion, and immune-complex-mediated tissue injury, which interact continuously with external triggers to shape disease expression (Tsokos, 2011; Crow, 2014; Kaul et al., 2016).
The CDF-Lupus™ Formula
For a given patient p, the CDF score is calculated across domains:
CDF_Lupus(p) = Σ [ w_k · D_k(p) · R_k · S_k · U_k(p) · M_k(p) ]
Where:
D_k(p) = Domain signal (0–1)
R_k = Reliability
S_k = Specificity
U_k(p) = Data usability
M_k(p) = Modifier, including environment, hormones, comorbidities, flare context, or structural barriers
w_k = Domain weight
Each domain produces a Domain Trust Score, and the final value reflects total lupus pattern alignment.
Domain Trust Calculation
For each domain:
T_k = D_k × R_k × S_k × U_k × M_k
C_k = w_k × T_k
Final:
CDF-Lupus(p) = Σ C_k
Interpretation Bands
≥ 0.75 → High-confidence lupus pattern
0.50–0.74 → Probable lupus pattern
0.30–0.49 → Early or partial autoimmune phenotype
< 0.30 → Low likelihood as primary driver
Diagnostic Fingerprint Calculation: Worked Example
Below is an illustrative example demonstrating how CDF-Lupus™ is applied in practice.
Patient Profile
Female, age 29
Persistent fatigue and joint pain
Photosensitivity and intermittent facial rash
Positive ANA, borderline anti-dsDNA
Episodes of brain fog and headaches
Mild anemia
Symptom flares triggered by stress and sun exposure
This presentation aligns with early or evolving lupus, where classification criteria are only partially met but disease processes may already be active.
Step 1: Domain Scoring
Domain | D_k | R_k | S_k | U_k | M_k | T_k | w_k | C_k |
Immune Activation and Autoantibody Profile | 0.72 | 0.88 | 0.82 | 0.85 | 0.90 | 0.397 | 0.18 | 0.0715 |
Inflammatory and Cytokine Signaling | 0.62 | 0.78 | 0.70 | 0.75 | 0.86 | 0.219 | 0.14 | 0.0307 |
Organ System Involvement | 0.68 | 0.82 | 0.76 | 0.80 | 0.88 | 0.298 | 0.16 | 0.0477 |
Neuroimmune and Cognitive Signal | 0.55 | 0.72 | 0.62 | 0.70 | 0.82 | 0.140 | 0.12 | 0.0168 |
Hematologic and Vascular Abnormalities | 0.45 | 0.78 | 0.70 | 0.80 | 0.78 | 0.153 | 0.10 | 0.0153 |
Metabolic and Mitochondrial Function | 0.42 | 0.68 | 0.55 | 0.70 | 0.80 | 0.088 | 0.08 | 0.0070 |
Environmental, Hormonal, and Structural Context | 0.78 | 0.82 | 0.72 | 0.86 | 0.92 | 0.365 | 0.22 | 0.0803 |
Step 2: Final Score Calculation
CDF-Lupus(p) = Σ C_k
= 0.0715
0.0307
0.0477
0.0168
0.0153
0.0070
0.0803
Final Score: 0.27
Interpretation
A score of 0.27 indicates:
Low-to-borderline early lupus pattern, with meaningful autoimmune signals that require monitoring rather than dismissal.
The model highlights signal concentration in:
immune activation and autoantibody profile
organ system involvement
environmental, hormonal, and structural context
inflammatory and cytokine signaling
This profile does not yet produce a probable lupus classification score, but it does suggest an evolving autoimmune pattern that may progress as additional symptoms, antibodies, hematologic findings, renal findings, or flare-linked organ involvement become clearer.
Clinical Implications
Monitor progression toward full classification criteria
Repeat antibody testing over time
Track photosensitivity, rash, joint symptoms, fatigue, and neurocognitive changes
Screen for renal, hematologic, and vascular involvement
Manage flare triggers, including UV exposure and stress
Consider early stabilization strategies before systemic burden worsens
Conclusion: Toward Earlier Lupus Recognition
Lupus is not inherently difficult to diagnose because it is rare, but because it evolves across time and systems in a way that traditional frameworks struggle to capture early. CDF-Lupus™ reframes lupus as a pattern recognition problem rather than a checklist. By integrating multi-domain signals into a composite diagnostic fingerprint, it enables earlier identification, better stratification, and more consistent recognition of systemic autoimmune disease. This approach aligns with a broader shift toward defining disease as a dynamic system state, where remission is characterized by stability, reduced flare probability, and functional recovery rather than the absence of isolated clinical markers (Yazdany and Schmajuk, 2014).
Within CYNAERA, this is reflected in the Remission Standard™, which evaluates remission as a multi-domain stability state rather than a binary outcome. This framework is further informed by The Eve Research Project, an ongoing, multi-phase research program examining how autoimmune symptoms evolve across hormonal life stages, environmental exposures, and flare patterns. By capturing longitudinal, real-world data, the project helps identify early system-level changes that often go unrecognized in traditional diagnostic models.
How to Cite this Paper
Adinig, C. (2026). CDF-Lupus™: Composite Diagnostic Fingerprint for Lupus. CYNAERA. Available at: https://www.cynaera.com/post/cdf-lupus
CYNAERA Framework Papers
This paper draws on a defined subset of CYNAERA Institute white papers that establish the methodological and analytical foundations of CYNAERA’s frameworks. These publications provide deeper context on prevalence reconstruction, remission, combination therapies and biomarker approaches. Our Long COVID Library, ME/CFS Library, Lyme Library, Autoimmune Library and CRISPR Remission Library are also in depth resources.
Author’s Note
All insights, frameworks, and recommendations in this written material reflect the author's independent analysis and synthesis. References to researchers, clinicians, and advocacy organizations acknowledge their contributions to the field but do not imply endorsement of the specific frameworks, conclusions, or policy models proposed herein. This information is not medical guidance.
Patent-Pending Systems
Bioadaptive Systems Therapeutics™ (BST) and affiliated CYNAERA frameworks are protected under U.S. Provisional Patent Application No. 63/909,951. CYNAERA is built as modular intelligence infrastructure designed for licensing, integration, and strategic deployment across health, research, public sector, and enterprise environments.
Licensing and Integration
CYNAERA supports licensing of individual modules, bundled systems, and broader architecture layers. Current applications include research modernization, trial stabilization, diagnostic innovation, environmental forecasting, and population level modeling for complex chronic conditions. Basic licensing is available through CYNAERA Market, with additional pathways for pilot programs, institutional partnerships, and enterprise integration.
About the Author
Cynthia Adinig is the founder of CYNAERA, a modular intelligence infrastructure company that transforms fragmented real world data into predictive insight across healthcare, climate, and public sector risk environments. Her work sits at the intersection of AI infrastructure, federal policy, and complex health system modeling, with a focus on helping institutions detect hidden costs, anticipate service demand, and strengthen planning in high uncertainty environments.
Cynthia has contributed to federal health and data modernization efforts spanning HHS, NIH, CDC, FDA, AHRQ, and NASEM, and has worked with congressional offices including Senator Tim Kaine, Senator Ed Markey, Representative Don Beyer, and Representative Jack Bergman on legislative initiatives related to chronic illness surveillance, healthcare access, and data infrastructure. In 2025, she was appointed to advise the U.S. Department of Health and Human Services and has testified before Congress on healthcare data gaps and system level risk.
She is a PCORI Merit Reviewer, currently advises Selin Lab at UMass Chan, and has co-authored research with Harlan Krumholz, MD, Akiko Iwasaki, PhD, and David Putrino, PhD, including through Yale’s LISTEN Study. She also advised Amy Proal, PhD’s research group at Mount Sinai through its CoRE advisory board and has worked with Dr. Peter Rowe of Johns Hopkins on national education and outreach focused on post-viral and autonomic illness. Her CRISPR Remission™ abstract was presented at CRISPRMED26 and she has authored a Milken Institute essay on artificial intelligence and healthcare.
Cynthia has been covered by outlets including TIME, Bloomberg, Fortune, and USA Today for her policy, advocacy, and public health work. Her perspective on complex chronic conditions is also informed by lived experience, which sharpened her commitment to reforming how chronic illness is understood, studied, and treated. She also advocates for domestic violence prevention and patient safety, bringing a trauma informed lens to her research, systems design, and policy work. Based in Northern Virginia, she brings more than a decade of experience in strategy, narrative design, and systems thinking to the development of cross sector intelligence infrastructure designed to reduce uncertainty, improve resilience, and support institutional decision making at scale.
References
Aringer, M., Costenbader, K., Daikh, D., et al. (2019). 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Annals of the Rheumatic Diseases, 78(9), 1151–1159.
Bertsias, G., Cervera, R. and Boumpas, D.T. (2012). Systemic lupus erythematosus: pathogenesis and clinical features. EULAR Textbook on Rheumatic Diseases, 476–505.
Crow, M.K. (2014). Type I interferon in the pathogenesis of lupus. Journal of Immunology, 192(12), 5459–5468.
Fanouriakis, A., Kostopoulou, M., Alunno, A., et al. (2019). 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Annals of the Rheumatic Diseases, 78(6), 736–745.
Kaul, A., Gordon, C., Crow, M.K., et al. (2016). Systemic lupus erythematosus. Nature Reviews Disease Primers, 2, 16039.
Lisnevskaia, L., Murphy, G. and Isenberg, D. (2014). Systemic lupus erythematosus. The Lancet, 384(9957), 1878–1888.
Mosca, M., Tani, C., Carli, L. and Bombardieri, S. (2010). Undifferentiated connective tissue diseases (UCTD): simplified systemic autoimmune diseases. Autoimmunity Reviews, 10(5), 256–258.
Pisetsky, D.S., Spencer, D.M., Lipsky, P.E. and Rovin, B.H. (2018). Assay variation in the detection of antinuclear antibodies. Annals of the Rheumatic Diseases, 77(6), 911–913.
Rahman, A. and Isenberg, D.A. (2008). Systemic lupus erythematosus. New England Journal of Medicine, 358(9), 929–939.
Tsokos, G.C. (2011). Systemic lupus erythematosus. New England Journal of Medicine, 365(22), 2110–2121.
Yazdany, J. and Schmajuk, G. (2014). Quality of care in systemic lupus erythematosus. Current Opinion in Rheumatology, 26(5), 497–505.



Comments